Assessing Nurses’ Educational Needs based on Knowledge and Importance of Clinical Microbiology
Article information
Abstract
Purpose: The current study investigated how clinical microbiology courses are conducted at the undergraduate nursing level in South Korea to identify the perceptions of clinical nurses regarding their knowledge and the clinical importance of microbiology and further assess their educational needs. Methods: Curricula presented on the websites of 202 undergraduate nursing institutions were reviewed. In addition, a survey assessing the knowledge and importance of clinical microbiology perceived by nurses was conducted online. A total of 150 nurses participated in the survey. Data were analyzed using descriptive statistics, correlation coefficients, t-tests, analysis of variance, Borich Needs Assessment Model, and Locus for Focus Model. Results: The results indicated that 90% of undergraduate nursing institutions offer clinical microbiology courses under various subject names. The perceived knowledge and importance of clinical microbiology were correlated; however, knowledge was consistently lower than the perceived importance of clinical biology among nurses. The structure and proliferation of novel viruses ranked highest in the educational needs of nurses based on both the Borich Needs Assessment Model and Locus for Focus Model. Conclusion: Based on the findings, this study suggests educational opportunities for clinical microbiology in hospital settings to reduce discrepancies between knowledge and the importance of clinical microbiology faced by nurses.
INTRODUCTION
1. Background
Biological nursing science comprises integrating fundamental concepts of biological sciences in nursing science. The Korean Society of Biological Nursing Science (KSBNS) indicates that the biological nursing science curriculum should include the structures and functions of the human body, clinical microbiology, pathophysiology, and mechanisms and effects of drugs based on nursing models [1]. Although a holistic approach is stressed in nursing science, the most common health issue in clinical nursing practice is to address patients’ physical needs caused by illness. Biological nursing science aims to enable nurses to make clinical decisions through critical thinking by providing knowledge regarding etiology and the process of disease progression, accompanied by changes in physical structure and function, and treatment [2]. The Korean Accreditation Board of Nursing (KABON) recommends that biological nursing science should be offered as a fundamental course for nursing students [3]. In addition, more than 50% of nursing education programs administered by hospitals include biological nursing science [4]. It demonstrates that biological nursing science is an important subject matter not only to be taught at the undergraduate level but also be continued in practice in clinical settings.
Biological nursing science courses are prerequisites for nursing majors, and therefore, most biological nursing courses are offered in the freshman or sophomore years [5]. However, with changes in the university admission system, there are many students do not opt for biology and/or chemistry in high school, and they find the biological nursing science courses offered in early college unfamiliar and difficult [6,7]. It has been reported that grades in biological nursing courses had a positive impact on academic adjustment and that nursing students who were satisfied with their biological nursing science courses demonstrated higher levels of satisfaction in nursing major courses and clinical performance [7,8]. Additionally, biological nursing science knowledge acquired during undergraduate program builds the foundation for nurses to trust their clinical decision-making [9]. Therefore, the biological nursing science curriculum should be composed of the knowledge and methods frequently used in clinical practice and should be updated periodically to include the most recent research findings.
According to a study that surveyed courses on four fields of biological nursing science offered by 74 nursing educational institutions in South Korea in 2012, clinical microbiology courses were offered the least among the subfields [5]. A study analyzing the contents of nurse training programs administered in five tertiary hospitals reported that pathophysiology was taught most frequently, followed by structures and functions of the human body, and mechanisms and effects of drugs. Clinical microbiology is the least frequently taught course in nurse training programs [4]. In the 21st century, novel infectious diseases such as severe acute respiratory syndrome (SARS), novel influenza, the Middle East respiratory syndrome (MERS), and the coronavirus disease-2019 (COVID-19). Recent MERS outbreaks and COVID-19 pandemic that occurred in 2015 and 2020, respectively, highlight the importance of effectively responding to infectious diseases. As health-related laws for infection prevention, surveillance, and control are being reinforced, the role of nurses as infection control personnel has been emphasized [10]. Considering these changes in the healthcare environment, it is necessary to reexamine the curriculum of clinical microbiology.
A considerable discrepancy exists between clinical nurses’ perceived needs regarding different areas of clinical microbiology as identified in 2000 [11] and the standardized syllabus developed in 2013 by the KSBNS based on program outcomes [12]. In consideration of the central role played by nurses in controlling infectious diseases and healthcare-associated infection (HAI), it is necessary to assess the current status of the clinical microbiology curricula in nursing educational institutions, evaluate the clinical importance of the course content, and incorporate the findings to reinforce and revise the curricula for undergraduate students and educational programs for nurses.
2. Study purpose
The purposes of this study were to examine the current status of biological nursing science courses offered by nursing educational institutions, specifically clinical microbiology courses, and to assess clinical nurses’ perceptions of knowledge level and clinical importance of various clinical microbiology course contents. An additional purpose of this study was to provide evidence required for effective curriculum planning and execution. The specific objectives of this study were as follows:
To investigate the current status of clinical microbiology courses offered by nursing education institutions nationwide in South Korea.
To identify clinical nurses’ perceived knowledge level and clinical importance regarding clinical microbiology course content.
To identify clinical nurses’ educational needs regarding clinical microbiology curricula.
METHODS
1. Study design
This cross-sectional survey study aimed to examine the current status of clinical microbiology courses in nursing educational institutions in South Korea and identify clinical nurses’ perceived knowledge levels and clinical importance based on clinical microbiology course content.
2. Study subjects
To examine the current status of clinical microbiology curricula, courses taught in accredited colleges (as of December 28, 2021) listed on the KABON website were surveyed. Accordingly, the websites of 202 undergraduate nursing institutions were reviewed. Nine institutions were excluded from study because they did not offer any information on curricula, and a total of 193 were included in analysis.
A survey was conducted to investigate the clinical importance of clinical microbiology course content among clinical nurses working at hospitals. The participants voluntarily consented to participate in the online survey posted on the KSBNS website. The sample size was estimated using G*Power version 3.1 [13]. Under the assumptions of effect size (r)=.3, significance level (α)=.05, and power (1-β)=.95, the minimum sample size was estimated to be 138. Considering a dropout rate of 10%, a total of 150 participants were recruited to fill out the online survey and all 150 surveys were included for analysis.
3. Research instruments
The current status of the clinical microbiology curriculum: The analysis items for the curriculum included course title, course category, number of credits, lecture hours, laboratory/practicum hours, school year, and semester.
Knowledge and clinical importance of clinical microbiology course contents: The items regarding course content were developed based on clinical microbiology textbooks in and out of Korea and the syllabus developed by the KSBNS [12]. The final items were selected after content validity was confirmed by experts (a nursing professor with expertise in infection control and three nursing professors with experience in teaching clinical microbiology). To finalize the course content items, only those items with a content validity index (CVI) of 80% or higher were selected. The instrument was composed of 22 items across six domains of infection and immunity, pathogenic bacteria, pathogenic viruses, pathogenic fungi, infection prevention and control, and understanding of microbiological testing. For each item, participants were instructed to rate their knowledge level and clinical importance of clinical microbiology on a scale with a minimum score of 0 point and a maximum score of 10 points. The higher the score, the higher the perceived knowledge and clinical importance of the clinical microbiology course content. Cronbach’s α was .966 for knowledge and .974 for clinical importance.
4. Data collection
To collect data regarding the current status of clinical microbiology courses, the curriculum information on the website of each nursing educational institution was used. To collect data regarding the knowledge level and clinical importance of clinical microbiology course contents, the purpose and procedures of this study were posted on the KSBNS website to recruit participants for the survey. The survey was conducted using an online survey system and was designed such that the survey would begin once participants read the study description and clicked on the consent button. Personal identifying information was not collected, and the study data were stored in a password-protected computer in a researcher’s office. The data will be stored for three years after completion of the research and will be permanently deleted afterward.
5. Ethical consideration
The current study was approved by the institutional review board of D University located in Daejeon Metropolitan City (IRB No. 1040647-202108-HR-001-03), and data were collected between December 20, 2021, and January 7, 2022.
6. Data analysis
Survey data were analyzed using IBM SPSS Statistics (version 25.0; IBM, Chicago, IL) according to the study purpose and the characteristics of each variable, as follows:
The current status of clinical microbiology courses and participants’ general characteristics were analyzed by frequencies, percentages, means, and standard deviations.
The clinical importance of course contents were analyzed by means and standard deviations.
Perceived knowledge level and clinical importance of course contents by general characteristics were analyzed using independent t-tests and one-way analysis of variance (ANOVA). The variables that did not meet the normality assumption were analyzed using the Mann-Whitney and Kruskal-Wallis tests. The significant findings in the ANOVA or Kruskal-Wallis test were further analyzed by performing a post-hoc test with an independent t-test or Mann-Whitney test, depending on the normality test.
The correlation between total scores of knowledge and clinical importance was analyzed by Pearson’s correlation coefficient. For individual items, correlations were examined by computing Spearman’s rho statistics because the variables were single-item Likert scale scores.
Significance level was set at p<.05. In the multiple-comparison post-hoc test, Bonferroni correction was applied.
The educational needs were analyzed by the Borich Needs Assessment Model [14] and Locus for Focus Model [15]. The Borich Needs Assessment Model is based on the mean weighted discrepancy score (MWDS; [sum of (importance-knowledge)×mean importance]÷number of participants) to compute the discrepancy between the current knowledge level and importance weighted by item importance. The greater the value, the greater the educational need of the participant. The Locus for Focus Model is an approach for visualizing the need priorities. In the model, the items are displayed into four quadrants by the x- and y-axes, which display the mean importance values and discrepancies between importance and knowledge, respectively. The quadrant of high importance and high discrepancy (HH) indicates the items high in both importance and discrepancy; thus, these items are of the highest educational need. The quadrant of low importance and high discrepancy (LH) indicates the items low in importance but high in discrepancy; thus, these items have the second highest educational need. The quadrants of high importance and low discrepancy (HL) and low importance and low discrepancy (LL) indicate items with low educational needs. Items ranked high in both the Borich Needs Assessment Model and Locus for Focus Model are considered to have the highest educational need.
RESULTS
1. Status of currently offered clinical microbiology courses
1) Course titles
The curricula offered in 193 nursing schools were examined, and 173 (89.6%) included clinical microbiology courses in their nursing curricula. Thirty-five different titles for clinical microbiology identified in the 173 schools. The frequency of “microbiology” in the course title was the highest, offered in 64 schools (37.0%), followed by “clinical microbiology” in 20 schools (11.6%), “microorganisms and infection control” in 19 schools (11.0%), “infection microorganisms and nursing” in 17 schools (9.8%), “microorganisms and infection” and “infection control” in seven schools each (4.0%), “infection microbiology” in six schools (3.5%), “nursing microbiology” in three schools (1.7%), and “infection control and microbiology,” “microbiology and practice,” and “hospital microorganisms and infection control” in two schools each (1.2%; Table 1).

Course Titles for Clinical Microbiology Courses (N=173)
2) Course category, number of credits, hours of lecture and laboratory/practicum, and semester
Clinical microbiology courses were classified as major fundamental courses in 101 schools (58.4%), as major elective courses in 29 schools (16.8%), and as major essential courses in 21 schools (12.1%). Additionally, the courses were classified into various categories including undergraduate fundamental, major, fundamental, and others in different schools. Regarding the number of credits, most schools (n=147, 85.0%) had a 2-credit course. Most schools (n=143, 82.7%) offered two-hour classes for theory lectures, whereas only six schools (3.5%) offered the course as a laboratory or practicum. The course was most frequently offered in the 2nd semester of the sophomore year (n=77, 44.5%), followed by the 2nd semester of the freshman year (n=67, 38.7%), and the 1st semester of the freshman year (n=14, 8.1%) (Table 2).
Curriculum Characteristics of Clinical Microbiology Courses (N=173)
2. Clinical nurses’ perceived clinical microbiology knowledge and clinical importance of clinical microbiology
Of the total participants who took the survey, 96% were female. The mean age of all participants was 35±8.63 and the age group of 30 years or younger was the highest (36.7%) of all age groups (Table 3). Regarding educational level, a baccalaureate degree was the most common (61.3%). Most participants worked at a tertiary hospital (72.7%) and a hospital with 500-999 beds (52.7%), and were staff nurses (78.0%). The total duration of the participants’ clinical experience was 134±96.04 months. The most common current working department was the general ward (49.3%) and 75.3% of the participants took a clinical microbiology course during their undergraduate study. Knowledge and clinical importance were not statistically significantly different according to participants’ general characteristics except differences in clinical importance according to education level (χ2=9.88, p=.007; Table 3). The clinical importance of clinical microbiology was rated higher in participants with a master’s degree or above (7.47±1.83) than in participants with a diploma (5.70±1.49).
Clinical Microbiology Knowledge and Importance according to Participant Characteristics (N=150)
Overall, the mean knowledge score was 5.25±1.60 and the mean importance score was 7.15±1.68. With respect to knowledge, the top three items comprised guidelines for infection prevention and control (item 21, 7.41±1.99), disinfection and sterilization (item 20, 7.41±2.08), and general principles of sampling for microbiological testing (item 22, 6.96±2.25). The bottom three items were characteristics of Neisseria bacteria (item 8, 3.9±1.87), the structure and proliferation of non-enveloped RNA virus (item 16, 3.93±1.96), and the structure and proliferation of enveloped RNA virus (item 15, 4.07±2.03; Table 4). With respect to clinical importance, the top three items were guidelines for infection prevention and control (item 21, 8.87±1.66), disinfection and sterilization (item 20, 8.69±1.90), and general principles of sampling for microbiological testing (item 22, 8.55±1.77), while the bottom three items were characteristics of Neisseria bacteria (item 8, 6.11±2.17), the structure and proliferation of non-enveloped DNA virus (item 14, 6.33±2.16), and the structure and proliferation of enveloped DNA virus (item 13, 6.41±2.19).

Correlation and Discrepancy between Knowledge and Importance of Clinical Microbiology
The correlation between total knowledge and clinical importance scores was positive and statistically significant (r=.30, p<.001). The knowledge and clinical importance scores for all participants showed positive correlations. The discrepancy between knowledge level and clinical importance was statistically significant for all the items (Table 4). The items for which the discrepancy was significant at the highest level were the structure and proliferation of novel viruses (item 18, Z=9.03, p<.001), structure and proliferation of hepatitis virus (item 17, Z=9.01, p<.001), and structure and proliferation of non-enveloped RNA (item 16, Z=8.70, p<.001). However, in the MWDS-based analysis, the structure and proliferation of novel viruses (item 18, MWDS=20.34, educational need rank=1st) showed the greatest discrepancy, followed by the structure and proliferation of hepatitis virus (item 17, MWDS=18.50, educational need rank=2nd), and the structure and proliferation of pathologic fungi (item 19, MWDS=15.95, educational need rank=3rd).
According to the results of the analysis by the Locus for Focus model (Figure 1), the items located in HH quadrant were the structure and proliferation of novel viruses (item 18) and disorders by hypersensitivity types (item 4). The following items were located in the LH: difference between staphylococci and streptococci (item 7), characteristics of Neisseria bacteria (item 8), structure and proliferation of enveloped DNA virus (item 13), structure and proliferation of non-enveloped DNA virus (item 14), structure and proliferation of enveloped RNA virus (item 15), structure and proliferation of non-enveloped RNA virus (item 16), structure and proliferation of hepatitis virus (item 17), and structure and proliferation of pathologic fungi (item 19). The following items were located in the LL quadrant: difference between innate and acquired immunity (item 2), vaccine mechanism and response (item 5), differences between Gram-positive and Gram-negative bacteria (item 6), characteristics of pathogenic Escherichia coli (item 9), characteristics of anaerobic bacteria (item 10), and characteristics of acid-fast bacteria (item 11), whereas immune responses (item 1), characteristics by hypersensitivity types (item 3), actions and resistance of antibiotics (item 12), disinfection and sterilization (item 20), guidelines for infection control and prevention (item 21), and general principles of sampling for microbiological testing (item 22) were located in the HL quadrant.
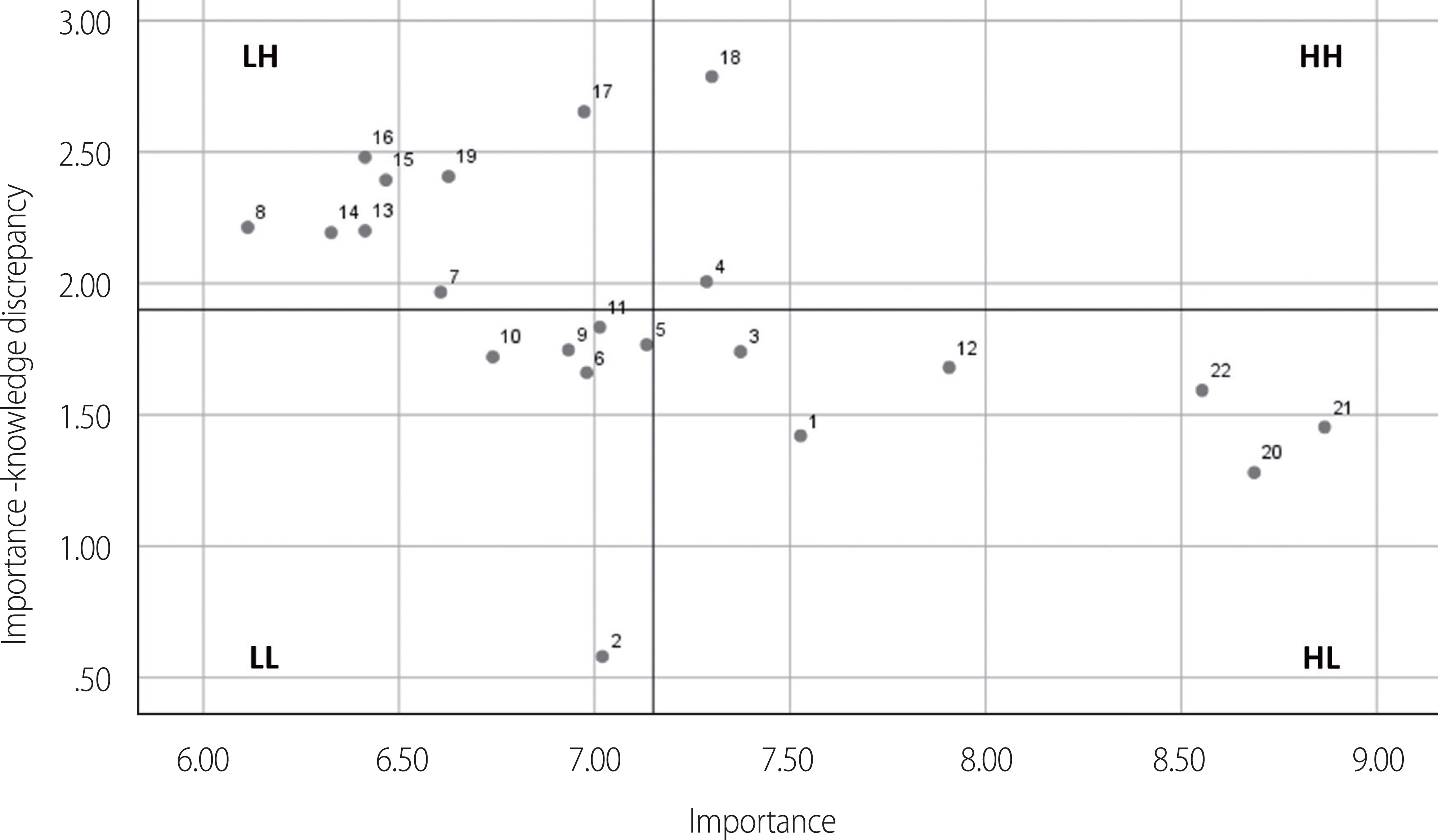
Locus for focus model. HH=High importance and high discrepancy; HL=High importance and low discrepancy; LH=Low importance and high discrepancy; LL=Low importance and low discrepancy.
Of the items ranked first through tenth in the Borich Needs Assessment Model based on MWDS, items 4, 8, 13, 14, 15, 16, 17, 18, and 19 were in HH (top priority in educational need) or LH (2nd highest priority) in the Locus for Focus model. Although characteristics of pathogenic Escherichia coli (item 9) ranked second in the Borich needs assessment model, it was considered to have a low educational need because it was high in importance but low in discrepancy. The structure and proliferation of novel viruses (item 18) showed the highest educational need in both the Borich Needs Assessment Model and the Locus for Focus Model (Table 4 and Figure 1).
DISCUSSION
The present study was conducted to examine the current status of clinical microbiology courses offered in nursing educational institutions in South Korea, investigate clinical nurses’ perceived knowledge level and clinical importance of various microbiology course contents, examine the correlations and discrepancies between knowledge level and clinical importance, and prioritize clinical microbiology course contents in terms of nurses’ educational needs.
Of the 202 undergraduate nursing institutions listed on the KABON website, the curricula of 193 schools were examined. Of the 193 schools, 173 (89.6%) were found to offer courses in clinical microbiology. The most common course title was “microbiology,” offered in 64 schools (37.0%), followed by “clinical microbiology” (20 schools, 11.6%), “microorganisms and infection control” (19 schools, 11.0%), and “infection microorganisms and nursing” (17 schools, 9.8%). Terms such as “infection,” “infection control,” and “nursing” appeared frequently in the course titles, whereas in a previous study conducted in 2012, the most common course title across 74 four-year course universities was “microbiology” (35.1%), followed by “microbiology and practicum” (13.5%), and “clinical microbiology” (9.5%) [5]. Hence, it is speculated that the contents of clinical microbiology courses have expanded to include practical applications of the subject. Clinical microbiology courses were most frequently conducted as major fundamental courses (101 schools, 58.4%) as indicated in this study, a finding noticeably different from the 2012 study [5], which found that microbiology courses were operated as major essential or major elective courses in 48.7% of universities. The finding that the courses were commonly offered as a two-credit course in the 2nd semester of the freshman year or the 1st semester of the sophomore year was in line with the findings of the 2012 study [5]. However, in the present study, only six schools (3.5%) operated a practicum course, whereas, in the 2012 study, 15 schools (20.3%) did so. Future research should, therefore, investigate the effectiveness of clinical microbiology practicum courses, which can then be reflected in the development of a new curriculum.
The findings of the survey conducted in this study indicated that perceived knowledge of clinical microbiology was at a moderate level, with a mean of 5.25 out of 10 points. The perceived clinical importance was high, with a mean of 7.15. The correlation between knowledge and clinical importance was significant; however, compared to clinical importance, the current knowledge level was significantly low. Since there was no previous research to investigate knowledge and clinical importance of clinical microbiology, a direct comparison was infeasible. However, a few studies on biological nursing science conducted with nursing students and nurses reported low knowledge levels [16-20]. Additionally, the presence of a discrepancy between nurses’ perceptions of knowledge and importance regarding biological nursing science (pharmacology) has been reported. These findings are consistent with those of the current study [16]. These findings suggest that even though biological nursing science, including microbiology, is important in practice, nurses’ perceived knowledge level is lower than its importance. A domestic study found that the proportion of microbiology contents in education programs for nurses at tertiary hospitals was significantly low compared to other biological nursing science contents [4]. Similarly, a study conducted in the UK reported that nurses were not sufficiently educated on microbiology [21]. Therefore, microbiology education should be reinforced, both at the undergraduate level and in clinical practice in the future.
To identify the microbiology course contents of the highest priority, the Borich Needs Assessment Model and Locus for Focus Model were used. In the analysis based on the Locus for Focus model, 10 items were identified as the highest and the second-highest priorities for education. Two items were of top priority (in the HH quadrant) and eight additional items were in the LH quadrant, indicating the next highest priority items. Items of both high importance and high knowledge were not considered as high priority. Compared to the top 10 items in the Borich Needs Assessment Model, eight overlapping contents in both models were considered as high educational needs.
The top priority item in both models was “structure and proliferation of novel virus” (e.g., novel influenza, SARS-CoV-2, etc.). It suggests that the current level of knowledge regarding novel viruses does not reach the level of its clinical importance, despite the urgent educational needs. The importance of “structure and proliferation of novel virus” is high in this study due to the COVID-19 pandemic, which continues to impact lives globally. However, the finding that a high importance-knowledge discrepancy exists even two years after the pandemic was declared demonstrates that educational needs have not been met. Therefore, utmost priority should be dedicated to developing an efficient course on the structure of the proliferation of novel viruses, which will serve as a foundation for understanding diseases and developing interventions in the future.
Another course content in the HH quadrant (a top priority for education need) in the Locus for Focus Model and ranked high in the Borich Needs Assessment Model was “disorders by hypersensitivity type” in “infection and immunity.” This item is considered to be of high educational need as it was highly rated in clinical importance, however, the discrepancy between importance and knowledge was large. This item is included in the clinical microbiology syllabus developed by the KSBNS. It is also included in the content of “immune disorders” in pathophysiology syllabus [12]. There are various causes of hypersensitivity reactions, including microorganisms such as bacteria, viruses, and fungi. Hypersensitivity reactions, which are the mechanism of various diseases, have different therapeutic approaches because the immune mechanisms are different for each type [22]. Therefore, knowledge on mechanisms of hypersensitivity reaction and disorders is a critical foundation for understanding and applying effective nursing interventions.
All course contents regarding pathologic viruses and fungi were identified to be the second highest priority in the Locus for Focus Model and also ranked high in the Borich Needs Assessment Model. The item “structure and proliferation of novel virus” was high both in importance and in discrepancy, and thus, it was identified as a top priority for education. All other items regarding pathological viruses were the second-highest priority. Although participants rated the clinical importance of pathological virus-related items other than novel viruses at a moderate to high level, the importance level was lower than that of other items. Perceived knowledge was also lower for these items than for others, resulting in a large discrepancy between knowledge and importance. Thus, these contents need education. Viral disorders are treated with a variety of medications depending on the characteristics and proliferation of the virus [23]. Hence, it is important to understand not only the current novel viruses but also various other pathological viruses. Therefore, educational opportunities should be further expanded.
The importance of “characteristics of Neisseria bacteria” among pathologic bacteria was lower than any other microbiology content and the current knowledge level was the lowest too. Meningococcal meningitis and gonorrhea are infectious diseases caused by Neisseria bacteria. Meningococcal meningitis is one of Group 3 infectious diseases in South Korea. With the exception of some regions in Africa, it rarely occurs worldwide, affecting 3-30 persons per one million people, however, the mortality rate is high [24,25]. Gonorrhea is an infectious disease that affects 87 million people worldwide each year [26]. Hence, education on the “characteristics of Neisseria bacteria” should be reinforced in the curricula.
However, this does not mean that items with low priority in this study are not important or that education is not necessary. If the importance is high, but the current level of knowledge is already high, the gap between importance and knowledge reduces, and the priority of educational needs decreases. Therefore, the results of this study suggest that additional education on microbiological content with high importance-knowledge discrepancies is required, but in practice, all content of microbiology is important and should be included in the curriculum.
Biological nursing science knowledge is important for nurses in gaining trust and building positive relationships with patients and their families because it not only helps nurses understand and make sound decisions regarding nursing interventions but also aids them in simplifying and succinctly explaining nursing care and treatment [9]. In the future, research should be performed to unravel differences in knowledge acquisition according to different educational methods because many nursing students tend to perceive basic science courses as difficult [20,27], and there are wide variations in the number of class hours and teaching methods [18,27]. It has been suggested that nursing education should focus on its clinical significance [20]. Therefore, to promote the knowledge of microbiology, educational opportunities for nurses should be expanded, and simultaneously, effective teaching methods should be investigated.
CONCLUSION
This study found that most nursing education institutions in South Korea offer clinical microbiology courses in the curriculum for nursing students; however, clinical nurses perceived their knowledge to be lower than the clinical importance of clinical microbiology. In particular, the structure and proliferation of novel viruses and disorders by hypersensitivity types were high in both clinical importance and discrepancy between importance and knowledge; hence, these areas have been identified as a high priority for education. The content that clinical nurses perceive as important in practice should be included in undergraduate microbiology courses, and up-to-date findings in the field of clinical microbiology should continue to be taught at hospitals. The current study findings are of significance in that they present data helpful in designing a comprehensive undergraduate curriculum and developing hospital educational programs. An additional significance of this study is that visualization of educational needs was attempted using the Locus for Focus Model, and it is suggested that the model be applied in studies in other biological nursing fields.
CONFLICT OF INTERREST
The authors state that they have no conflicts of interest to declare.
AUTHORSHIP
JLL and YJ contributed to the conception and design of the study. Both authors contributed to the data collection, performed the statistical analysis and interpretation, and wrote the manuscript. All authors have read and approved the final manuscript.