


žĄú Ž°†
1. žóįÍĶ¨žĚė ŪēĄžöĒžĄĪ
ž†Ą žĄłÍ≥Ą žĚłÍĶ¨žĚė 70%ŽäĒ ŪŹČžÉĚ Ūēú Ž≤ą žĚīžÉĀžĚė žôłžÉĀ žā¨ÍĪī(traumatic events)žĚĄ Í≤ĹŪóėŪēúŽč§. žôłžÉĀ ŪõĄ žä§Ū䳎†ąžä§ žě•žē†(Post-Traumatic Stress Disorder, PTSD)ŽäĒ žôłžÉĀžĚĄ Í≤ĹŪóėŪēú žĚīŪõĄ žĻ®Ūą¨žôÄ ŪöĆŪĒľ, žĚłžßÄ ŽįŹ ÍłįŽ∂ĄžĚė Ž∂Äž†ēž†ĀžĚł Ž≥ÄŪôĒ, ÍįĀžĄĪ ŽįŹ ŽįėžĚĎžĄĪžĚė ŪėĄž†ÄŪēú Ž≥ÄŪôĒ ŽďĪžĚė ž¶ĚžÉĀžĚĄ Ž≥īžĚīŽäĒ žÉĀŪÉúŽ•ľ žĚėŽĮłŪēúŽč§[1-3]. ÍĶ≠ŽāīžĚė Í≤Ĺžöį, ŽßĆ 18-64žĄł žĄĪžĚłžĚė 1.6% (Žā®žĄĪ 1.0%, žó¨žĄĪ 2.1%)ÍįÄ ŪŹČžÉĚ 1Ž≤ą žĚīžÉĀ PTSD žßĄŽč®žĚĄ ŽįõŽäĒ Í≤ÉžúľŽ°ú žēĆŽ†§ž†ł žěąžúľŽ©į, žĚľŽ≥ł 1.3%, ŽŹôžú†ŽüĹ 2.4%, žĄúžú†ŽüĹ 4%, ŽĮłÍĶ≠ 6.8%, žļźŽāėŽč§ 9.2% ŽďĪ žĄłÍ≥Ąž†ĀžúľŽ°ú Žč§žĖĎŪēú PTSD ŪŹČžÉĚ žú†Ž≥ĎŽ•†žĚī Ž≥īÍ≥†ŽźėžóąŽč§[4-7]. žēĹ 80-90%žĚė PTSD ŪôėžěźŽäĒ žöįžöłžě•žē†, Ž∂ąžēąžě•žē†, žěźžāīžúĄŪóė, ŪēīŽ¶¨žúĄŪóė, Ž¨ľžßąžā¨žö©žě•žē†Ž•ľ ŽŹôŽįėŪēėÍ≥†[1,4], ŽĆĞ̳ÍīÄÍ≥ĄžôÄ žßĀžě•žÉĚŪôúžĚĄ ŪēėŽäĒŽćį žĖīŽ†§žõĞ̥ Í≤™žĚĄ ŽŅźŽßĆ žēĄŽčąŽĚľ ŽßĆžĄĪ žßąŪôė žúĄŪóė ž¶ĚÍįÄ, ŽÖłŪôĒ ÍįÄžÜćŪôĒ ŽįŹ ž°įÍłį žā¨ŽßĚ ž¶ĚÍįÄžôÄŽŹĄ žóįÍīÄžĄĪžĚī Ž≥īÍ≥†Žźú ŽįĒ žěąŽč§[4,8].
žĶúÍ∑ľ žôłžÉĀ ŪõĄ žä§Ū䳎†ąžä§ žě•žē†žĚė žĻėŽ£Ć žēĹŽ¨ľŽ°ú žė•žčúŪ܆žč†(oxytocin)žĚė ŽĻĄÍįēŪą¨žó¨ÍįÄ žčúŽŹĄŽźėÍ≥† žěąŽč§[1]. žė•žčúŪ܆žč†žĚÄ žĚłž≤ī žôłŽ∂ÄžôÄ ŽāīŽ∂ÄžĚė žěźÍ∑Ļ(žč¨Ž¶¨ž†ĀžĚł žä§Ū䳎†ąžä§ ŽďĪ)žóź ŽĆÄŪēú ŽįėžĚϞ̥ ž°įž†ąŪēėŽäĒ hypothalamic-pituitary-adrenal (HPA) axis ž§Ď žčúžÉĀŪēėŽ∂Ä(hypothalamus)žóźžĄú ŽßƎ吏ĖīžßÄŽäĒ žč†Í≤ĹŪėłŽ•īŽ™¨(neurohormone)žúľŽ°ú ž£ľŽ°ú žč§Žį©ŪēĶ(paraventricular nuclei)Í≥ľ žčúÍįĀŽ°úžúĄŪēĶ(supraoptic nuclei)žóźžĄú Ūē©žĄĪŽźėžĖī ŽáĆŪēėžąėž≤ī ŪõĄžóĹ(posterior pituitary)žĚīŽāė žč†Í≤ĹŽáĆŪēėžąėž≤ī(neurohypophysis)žóźžĄú Ūėąžē°žúľŽ°ú Ž∂ĄŽĻĄŽźúŽč§[9-13]. ŪĚĒŪěą žěźÍ∂Ā žąėž∂ēžĚĄ ŽŹĄžôÄ Ž∂ĄŽßƞ̥ žīȞߥŪēėÍ≥† Ž™®žú†Ž•ľ Ž∂ĄŽĻĄžčúŪā§ŽäĒ ŪėłŽ•īŽ™¨žúľŽ°ú žēĆŽ†§ž†ł žěąžßÄŽßĆ, žĚī žôłžóźŽŹĄ ŽáĆžĚė žó¨Žü¨ Ž∂ÄžúĄžóź žěĎžö©Ūēėžó¨ Ž∂ąžēąÍ≥ľ žä§Ū䳎†ąžä§Ž•ľ ÍįźžÜĆžčúŪā§Í≥† žĻú žā¨ŪöĆž†ĀžĚł ŪĖČŽŹôžĚĄ žīȞߥŪēėŽäĒ žěĎžö©žĚī Ž≥īÍ≥†ŽźėžóąŽč§[9-13]. žĚłž≤īŽäĒ žä§Ū䳎†ąžä§Ž•ľ ŽįõžúľŽ©ī žä§Ū䳎†ąžä§žóź ŽĆÄŪē≠ŪēėÍłį žúĄŪēī Ž∂Äžč†ŪĒľžßąžóźžĄú Ūėąžēē, Žß•Žįē, ŪėłŪĚ°žĚĄ ž¶ĚÍįÄžčúŪā§Í≥† Í∑ľžú°Í≥ľ ÍįźÍįĀ ÍłįÍīĞ̥ ŽĮľÍįźŪēėÍ≤Ć ŪēėŽäĒ žĹĒŽ•īŪčįžÜĒ(Cortisol)žĚĄ žÉĚžĄĪŪēėŽäĒŽćį[14], žė•žčúŪ܆žč†žĚÄ HPA axisžĚė žĚĆžĄĪ ŪĒľŽďúŽįĪžĚĄ ŪÜĶŪēī žĚī žĹĒŽ•īŪčįžÜĒ žąėžĻėŽ•ľ žä§Ū䳎†ąžä§Ž•ľ ŽįõÍłį ž†Ą žÉĀŪÉúŽ°ú Žāģž∂ĒÍ≥† žú†žßÄŪēėŽäĒ Žćį ÍīÄžó¨ŪēúŽč§Í≥† žēĆŽ†§ž†ł žěąŽč§[15]. ŽėźŪēú, žė•žčúŪ܆žč†žĚÄ Ūėźžė§žä§Žü¨žöī žěźÍ∑Ļžóź ŽĆÄŪēú Í≥ĶŪŹ¨/Ž∂ąžēą ŪĖČŽŹôÍ≥ľ ÍīÄŽ†®žĚī žěąŽäĒ Ū鳎ŹĄž≤ī(amygdala)žĚė ŽįėžĚĎžĄĪžĚĄ ÍįźžÜĆžčúŪā§Í≥†[16,17], žēąž†ē žčú(resting state), ŽĆÄŽáĆŪĒľžßąŽ≥ÄžóįÍ≥Ą(corticolimbic) žėĀžó≠Í≥ľžĚė žóįÍ≤įžĄĪžĚĄ ž¶ĚÍįÄžčúžľú Ž∂ąžēąÍ≥ľ Í≥ĶŪŹ¨Ž•ľ žôĄŪôĒžčúŪā§ŽäĒ Í≤ÉžúľŽ°ú žēĆŽ†§ž†łžěąŽč§[12,18,19]. Í≥ĶÍįź Žä•Ž†•[16,17]Í≥ľ Íįźž†ē žĚłžčĚ Žä•Ž†•[12,18,19]žĚĄ ŪĖ•žÉĀžčúŪā§Í≥†, ÍįúžĚł ÍįĄžĚė žč†ŽĘįžôÄ žē†žį©žĚĄ žīȞߥŪēėŽäĒ ŽďĪ žė•žčúŪ܆žč†žĚė žĻú žā¨ŪöĆž†Ā Ūö®Í≥ľÍįÄ žĄ†ŪĖČžóįÍĶ¨žóźžĄú Ž≥īÍ≥†ŽźėžóąŽč§[20].
PTSDžĚė žõźžĚłžĚī ŽźėŽäĒ ŽÜížĚÄ žä§Ū䳎†ąžä§Ž•ľ ž£ľŽäĒ žôłžÉĀ Í≤ĹŪóėžĚÄ HPA axisžôÄ žčúÍĶźžį®žÉĀŪēĶ(suprachiasmatic nucleus)žóź žėĀŪĖ•žĚĄ ž£ľžĖī ŽāīžĚłžĄĪ žė•žčúŪ܆žč†žĚė Ūē©žĄĪÍ≥ľ Žį©ž∂úžĚĄ ÍįźžÜĆžčúŪā§ŽäĒ Í≤ÉžúľŽ°ú žēĆŽ†§ž°ĆŽč§[21,22]. ŽāīžĚłžĄĪ žė•žčúŪ܆žč†žĚė ÍįźžÜĆŽäĒ HPA axisžĚė žĹĒŽ•īŪčįžÜĒžóź ŽĆÄŪēú žĚĆžĄĪ ŪĒľŽďúŽįĪžĚĄ žēĹŪôĒžčúžľú Í≥†žĹĒŽ•īŪčįžÜĒŪėąž¶Ě(hypercortisolemia)žĚī žú†ŽįúŽźėÍ≥†, Ū鳎ŹĄž≤īŽ•ľ Í≥ľŪôúžĄĪŪôĒžčúžľú žä§Ū䳎†ąžä§ žěźÍ∑Ļžóź Í≥ľŽŹĄŪēú ŽįėžĚϞ̥ Ž≥īžĚīÍ≤Ć ŪēúŽč§ [23,24]. žĶúÍ∑ľ, ŽĻĄÍįēžĚĄ ŪÜĶŪēú žôłžĚłžĄĪ žė•žčúŪ܆žč†žĚė Ūą¨žó¨ŽäĒ PTSDŽ•ľ žßĄŽč®ŽįõÍĪįŽāė ž†ēžč†ž†Ā žôłžÉĀžĚĄ Í≤™žĚÄ ŽĆÄžÉĀžěźžóźÍ≤Ć žä§Ū䳎†ąžä§žóź ŽĆÄŪēú ŪėłŽ•īŽ™¨ž†Ā¬∑ž£ľÍīÄž†Ā ŽįėžĚϞ̥ ÍįźžÜĆžčúŪā§Í≥†, žč†ž≤ī Ūē≠žÉĀžĄĪžĚĄ ŪöĆŽ≥ĶžčúŪā§Ž©į[25], Íįźž†ē žĚłžčĚ, ŽĆĞ̳ÍīÄÍ≥Ą, žč†ŽĘį ŽįŹ žĻú žā¨ŪöĆž†Ā ŪĖČŽŹôÍ≥ľ ÍįôžĚÄ žā¨ŪöĆž†Ā žĚłžčĚ Žä•Ž†•žĚĄ ÍįúžĄ†ŪēėŽäĒ Í≤ÉžúľŽ°ú Ž≥īÍ≥†ŽźėžóąŽč§[3,26-28].
ŪėĄžě¨ PTSDžĚė žĻėŽ£ĆžóźŽäĒ žēĹŽ¨ľžĻėŽ£ĆŽ≥īŽč§ žč¨Ž¶¨žĻėŽ£ĆÍįÄ ŽćĒ Ūö®Í≥ľž†ĀžĚīÍ≥† žöįžĄ†ž†ĀžĚł žĻėŽ£ĆŽ°ú Í≥†Ž†§ŽźėÍ≥† žěąŽč§[29,30]. Í≤ĹŪóėž†Ā Í∑ľÍĪįÍįÄ žěė ŪôēŽ¶ĹŽźú žč¨Ž¶¨žĻėŽ£ĆŽäĒ žĚłžßÄŪĖČŽŹôžĻėŽ£Ć(cognitive behavioral therapy, CBT), žĚłžßÄž≤ėŽ¶¨žĻėŽ£Ć(cognitive processing therapy, CPT), žĚłžßÄžĻėŽ£Ć(cognitive therapy, CT), žßÄžÜćŽÖłž∂úžĻėŽ£Ć(Prolonged Exposure, PE)Ž•ľ ŪŹ¨Ūē®Ūēú ŽÖłž∂úžĻėŽ£Ć ŽďĪžĚī žěąÍ≥†, žēąÍĶ¨žöīŽŹô ŽĮľÍįźŪôĒ žÜĆžč§ ŽįŹ žě¨ž≤ėŽ¶¨(eye movement desensitization and reprocessing, EMDR)žôÄ ŽāīŽü¨ŪčįŽłĆ ŽÖłž∂úžĻėŽ£Ć(Narrative Exposure Therapy, NET)ŽŹĄ Ūö®Í≥ľž†ĀžĚł žĻėŽ£ĆŽ°ú ÍįĄž£ľŽźúŽč§[29,30]. ŽĮłÍĶ≠ žč¨Ž¶¨ŪēôŪöĆ(American Psychological Association, APA)žĚė 2017ŽÖĄ PTSD žĻėŽ£Ć ÍįÄžĚīŽďúŽĚľžĚłžóź ŽĒįŽ•īŽ©ī, fluoxetine, paroxetine, sertraline ŽďĪžĚė žĄ†ŪÉĚž†Ā žĄłŽ°úŪ܆ŽčĆ žě¨ŪĚ°žąė žĖĶž†úž†ú(Selective serotonin reuptake inhibiotors, SSRIs)žôÄ venlafaxine ÍįôžĚÄ žĄłŽ°úŪ܆ŽčĆ ŽįŹ ŽÖłŽ•īžóźŪĒľŽĄ§ŪĒĄŽ¶į žě¨ŪĚ°žąė žĖĶž†úž†ú(Serotonin and norepinephrine reuptake inhibitors, SNRIs) ŽďĪžĚī PTSD žĻėŽ£ĆžēĹŽ¨ľŽ°ú Í∂ĆÍ≥†ŽźėÍ≥† žěąŽč§. žč¨Ž¶¨žĻėŽ£Ć(CBT, CPT, CT, PE)ÍįÄ ÍįēŽ†•Ūěą Í∂ĆÍ≥†ŽźėÍ≥† žěąŽäĒ Í≤Éžóź ŽįėŪēī, PTSD žĻėŽ£ĆžēĹŽ¨ľžĚÄ Í∑ľÍĪįÍįÄ Ž∂ąž∂©Ž∂ĄŪēėžó¨ ž°įÍĪīžóź ŽĒįŽĚľ Í∂ĆÍ≥†ŽźėŽäĒ ‚ÄėŽ≥īŪÜĶ(moderate)‚ÄôžĚė ÍįēŽŹĄŽ°ú Í∂ĆÍ≥†ŽźėÍ≥† žěąŽč§[31]. Í∑łŽü¨Žāė, ŪėĄžě¨ žč¨Ž¶¨žĻėŽ£ĆÍįÄ 1/3 ž†ēŽŹĄžĚė ŪôėžěźžóźžĄúŽäĒ Ūö®Í≥ľÍįÄ žóÜÍ≥†, Í≤Ĺž†úž†Ā, žčúÍįĄž†ĀžĚł Ž¨łž†úŽ°ú žč¨Ž¶¨žĻėŽ£ĆŽ•ľ žßÄžÜćŪēėÍłį žĖīŽ†ĶÍĪįŽāė Í∑ľÍĪįÍłįŽįėžĻėŽ£ĆŽ•ľ ž†úÍ≥ĶŪē† žąė žěąŽäĒ žßÄžó≠žā¨ŪöĆ Žāī ž†ĄŽ¨łÍįÄ Ž∂Ğ쨎äĒ žč¨Ž¶¨žĻėŽ£ĆžĚė ž£ľŽźú ž†úŪēúžöĒžĚłžúľŽ°ú žěĎžö©ŪēúŽč§[32,33]. ŽĒįŽĚľžĄú, PTSD žĻėŽ£ĆŽ•ľ žúĄŪēú Ūö®Í≥ľž†ĀžĚł žēĹŽ¶¨Ūēôž†Ā ž§Ďžě¨ ÍįúŽįú ŪēĄžöĒžĄĪžĚÄ žßÄžÜ枆ĀžúľŽ°ú ž¶ĚÍįÄŪēėÍ≥† žěąŽč§[34].
PTSD ŪôėžěźŽ•ľ ŽĆÄžÉĀžúľŽ°ú žė•žčúŪ܆žč†žĚĄ žĚľŪöĆ Ūą¨žó¨Ūēú ŽÖľŽ¨łžĚĄ ž≤īÍ≥Ąž†Ā Ž¨łŪóĆ Í≥†žįįŪēú Giovanna ŽďĪ[35]žĚė žóįÍĶ¨žóźžĄúŽäĒ žė•žčúŪ܆žč† Ūą¨žó¨ÍįÄ ÍĶźÍįźžč†Í≤Ĺ ŪôúžĄĪŽŹĄ(sympathetic tone)žôÄ žĹĒŽ•īŪčįžÜĒ(cortisol) žąėž§ÄžĚĄ ÍįźžÜĆžčúŪā§Í≥† ŽáĆ ÍłįŽä•žĚĄ ÍįúžĄ†žčúŪā§ŽäĒ ŽďĪ, PTSD ž¶ĚžÉĀžĚė žĻėŽ£Ć Ūö®Í≥ľ ÍįÄŽä•žĄĪžĚĄ ŪôēžĚłŪĖąŽč§. Í∑łŽü¨Žāė, žĄ†ŪĖČžóįÍĶ¨ŽäĒ žė•žčúŪ܆žč†žĚĄ žĚľŪöĆžĄĪžúľŽ°ú Ūą¨žó¨Ūēú žóįÍĶ¨ŽßĆ ŪŹ¨Ūē®Ūēėžó¨, Žč§ŪöĆ Ūą¨žó¨Ž•ľ ŪēĄžöĒŽ°ú ŪēėŽäĒ žēĹŽ¨ľžĻėŽ£ĆžĚė Ūö®Í≥ľŽ°ú žĚľŽįėŪôĒŪēėÍłį žĖīŽ†§žöī ž†úŪēúž†źžĚĄ ÍįÄžßÄÍ≥† žěąŽč§. ŽĒįŽĚľžĄú Ž≥ł žóįÍĶ¨žóźžĄúŽäĒ PTSD ž¶ĚžÉĀžĚĄ ÍįĞߥ ŽĆÄžÉĀžěźžóźÍ≤Ć žė•žčúŪ܆žč†žĚĄ žĚľŪöĆ ŽėźŽäĒ Žč§ŪöĆ Ūą¨žó¨Ūēú ŽÖľŽ¨łžĚĄ Ž¨łŪóĆÍ≥†žįį Ūēėžó¨, PTSD žĻėŽ£Ćž†úŽ°úžĄú žė•žčúŪ܆žč† ŽĻĄÍįēŪą¨žó¨žĚė ÍįÄŽä•žĄĪžĚĄ ŪôēžĚłŪēėÍ≥†žěź ŪēúŽč§. ŽėźŪēú ž†ĄŽ¨ł žĚėŽ£ĆžĚłžĚī žąėŪĖČŪēėŽäĒ ž†ēŽß• ž£ľžěÖ ŽďĪžĚī žēĄŽčĆ, ŽĻĄÍįēžĚĄ ŪÜĶŪēī žěźÍįÄ Ūą¨žó¨Ūē† žąė žěąŽč§ŽäĒ ž†źžóźžĄú PTSD Ūôėžěźžóź ŽĆÄŪēú ÍįĄŪėł žąėŪĖČžĚė Ž≥Ķžě°žĄĪžĚĄ Žāģž∂ú žąė žěąŽč§. žĚīŽ°úžć® ŽćĒžöĪ Ūö®Í≥ľž†ĀžĚł ÍįĄŪėł ž§Ďžě¨Ž•ľ žĄ§Í≥ĄŪē† žąė žěąŽč§ŽäĒ žł°Ž©īžóźžĄú žė•žčúŪ܆žč†žĚĄ Žč§ŪöĆ ŽĻĄÍįē Ūą¨žó¨ŪēėŽäĒ Í≤ÉžĚė Ūö®Í≥ľžĄĪžĚĄ ŪôēžĚłŪē† ŪēĄžöĒÍįÄ žěąŽč§.
2. žóįÍĶ¨žĚė Ž™©ž†Ā
Ž≥ł žóįÍĶ¨ŽäĒ PTSDžóź ŽĆÄŪēú žė•žčúŪ܆žč†žĚė Ūą¨žó¨ž°įÍĪīÍ≥ľ Í∑ł žĻėŽ£ĆŪö®Í≥ľŽ•ľ ŪĆĆžēÖŪē®žúľŽ°úžć® žė•žčúŪ܆žč†žĚė žôłžÉĀ ŪõĄ žä§Ū䳎†ąžä§ žě•žē†žĚė žĻėŽ£Ćž†úŽ°úžĄúžĚė ÍįÄŽä•žĄĪžĚĄ ŪôēžĚłŪēėÍ≥†žěź ŪēúŽč§. žĚīŽ•ľ žúĄŪēú ÍĶ¨ž≤īž†ĀžĚł žóįÍĶ¨ Ž™©ž†ĀžĚÄ Žč§žĚĆ Í≥ľ ÍįôŽč§.
3. žóįÍĶ¨ Žį©Ž≤ē
1) žóįÍĶ¨ žĄ§Í≥Ą
Ž≥ł žóįÍĶ¨ŽäĒ PTSD žßĄŽč®žĚĄ ŽįõžēėÍĪįŽāė, žôłžÉĀž†Ā žā¨ÍĪīžóź ŽÖłž∂úŽźú žįłÍįĞ쟎•ľ ŽĆÄžÉĀžúľŽ°ú žė•žčúŪ܆žč† Ūą¨žó¨ž°įÍĪīÍ≥ľ Í∑ł Ūö®Í≥ľžôÄ ÍīÄŽ†®Žźú žóįÍĶ¨ ŽŹôŪĖ•žĚĄ Ž∂ĄžĄĚŪēėÍłį žúĄŪēú ž≤īÍ≥Ąž†Ā Ž¨łŪóĆÍ≥†žįį žóįÍĶ¨žĚīŽč§.
2) Ž¨łŪóĆ žĄ†ž†ēÍłįž§ÄÍ≥ľ ž†úžôłÍłįž§Ä
Ž¨łŪóĆ Í≤ÄžÉČžĚÄ 2021ŽÖĄ 1žõĒ 20žĚľŽ∂ÄŪĄį 27žĚľÍĻĆžßÄ žĚīŽ£®žĖīž°ĆžúľŽ©į, 2021ŽÖĄ 1žõĒ 20žĚľ žĚīž†Ąžóź ŽįúÍįĄŽźú Ž™®Žď† žóįÍĶ¨ ŽÖľŽ¨łžĚĄ ŽĆÄžÉĀžúľŽ°ú Í≤ÄžÉČŪēėžėÄŽč§. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA)žĚė ÍįÄžĚīŽďúŽĚľžĚłžĚĄ ŽĒįŽĚľžĄú PubMed, PsycINFO, CINAHL ŽćįžĚīŪĄįŽ≤†žĚīžä§Ž•ľ Ūôúžö©ŪēėžėÄŽč§. ‚Äústress disorders, post-traumatic [MeSH Terms]‚ÄĚ, ‚Äúoxytocin [MeSH Terms]‚ÄĚ, ‚Äúclinical trial‚ÄĚ, ‚Äúplacebos [MeSH Terms]‚ÄĚ, ‚Äúrandomized controlled trial‚ÄĚ ŽďĪžĚė žėĀŽ¨ł Í≤ÄžÉČžĖīŽ•ľ žā¨žö©ŪēėžėÄŽč§. žĄ†ž†ēÍłįž§ÄžĚÄ Žč§žĚĆÍ≥ľ ÍįôŽč§. (1) PTSD žßĄŽč®žĚĄ ŽįõžēėÍĪįŽāė PTSDžóź ŽĆÄŪēú ž†ēžč†žě•žē†(Ž≥Ď) žßĄŽč®ŪÜĶÍ≥ĄŪ鳎ěĆ(Diagnostic and Statistical Manual of Mental Disorders, DSM)žĚė criterion AŽ•ľ ž∂©ž°ĪŪē† žąė žěąŽäĒ žôłžÉĀž†Ā žā¨ÍĪīžóź ŽÖłž∂úŽźú ŽßĆ 18žĄł žĚīžÉĀ ŽĆÄžÉĀžěź, (2) žė•žčúŪ܆žč†žĚĄ 1ŪöĆ žĚīžÉĀ Ūą¨žó¨ŪēėÍ≥†, (3) žěĄžÉĀžčúŪóė žóįÍĶ¨Ž•ľ žßĄŪĖČŪēú, (4) ŪēúÍĶ≠žĖī ŽėźŽäĒ žėĀžĖīŽ°ú ž∂úŪĆźŽźú žõźŽ¨ł ŪôēŽ≥īÍįÄ ÍįÄŽä•Ūēú, (5) Ž¨īžěĎžúĄŽĆÄž°įžčúŪóė(Randomized control trial, RCT) žóįÍĶ¨ŽßĆ ŪŹ¨Ūē®žčúžľįŽč§. ž†úžôłÍłįž§ÄžĚÄ (1) ŽĻĄžč§ŪóėžóįÍĶ¨žĚīÍĪįŽāė, (2) ŽßĆ 18žĄł ŽĮłŽßĆ žįłÍįĞ쟎•ľ ŽĆÄžÉĀžěźŽ°ú ŪēėÍĪįŽāė, (3) ŪēôžúĄŽÖľŽ¨łžĚīŽāė, (4) žīąŽ°ĚŽßĆ ž°īžě¨ŪēėŽäĒ ŽÖľŽ¨łžĚÄ ž†úžôłŪēėžėÄŽč§.
3) Ž¨łŪóĆ Í≤ÄžÉČ ŽįŹ žĄ†ž†ē
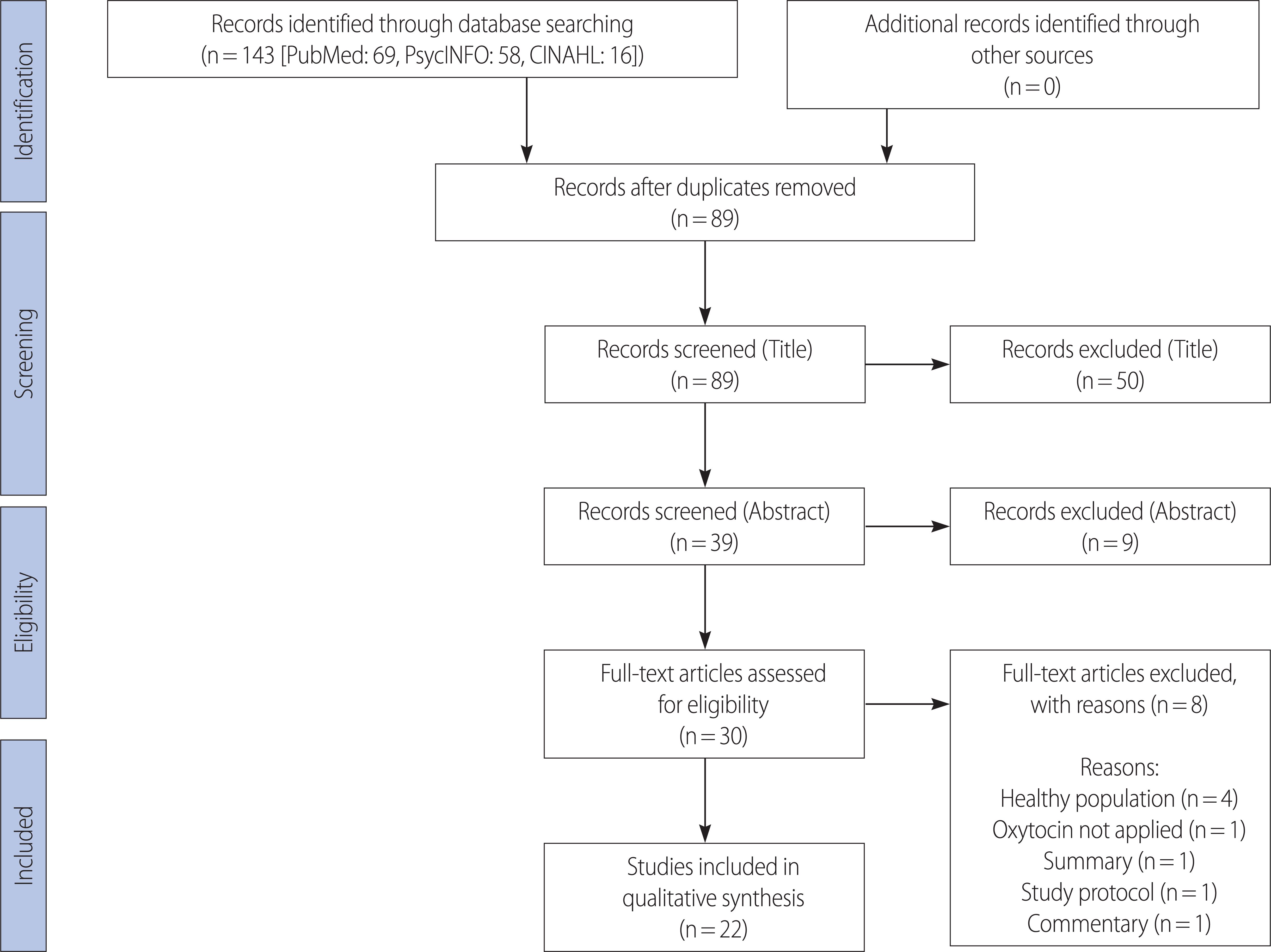
žóįÍĶ¨žěź ŽĎź Ž™ÖžĚī ŽŹôžĚľŪēú Ž¨łŪóĆ ž∂Ēž∂ú ŪėēžčĚžúľŽ°ú ŽćįžĚīŪĄįŽ≤†žĚīžä§žôÄ Í≤ÄžÉČ žóĒžßĄžĚĄ žĚīžö©Ūēėžó¨ Í≤ÄžÉČŪēėžėÄÍ≥†, Í≤ÄžÉČŽźú Ž¨łŪóƞ󟞥ú ž§ĎŽ≥Ķ ŽÖľŽ¨łžĚĄ ž†úÍĪįŪēú ŪõĄ žĄ†ž†ē ŽįŹ ž†úžôł Íłįž§Äžóź ŽĒįŽĚľ ŽÖľŽ¨łžĚė ž†úŽ™©, žīąŽ°Ě, žõźŽ¨łžĚĄ Žč®Í≥Ąž†ĀžúľŽ°ú Í≤ÄŪ܆ŪēėžėÄŽč§. Ž™®Žď† Žč®Í≥ĄŽäĒ ŽŹÖŽ¶Ĺž†ĀžúľŽ°ú žßĄŪĖČŪēú Ží§ žóįÍĶ¨ ŪöĆžĚėŽ•ľ ŪÜĶŪēī ŽĎź žóįÍĶ¨žěźžĚė Í≤įÍ≥ľ žĚľžĻė žó¨Ž∂ÄŽ•ľ ŪĆĆžēÖŪēėÍ≥† Žč§žĚĆ Žč®Í≥ĄŽ°ú žßĄŪĖČŪēėžėÄžúľŽ©į, žĚėÍ≤¨žĚī Ž∂ąžĚľžĻėŪēėŽäĒ Í≤Ĺžöį ž†ú 3žóįÍĶ¨žěźžôÄ ŪöĆžĚėŽ•ľ ŪÜĶŪēīžĄú Ūē©žĚė ŪõĄ žßĄŪĖČŪēėžėÄŽč§. Í≤ÄžÉČŽźú Ž¨łŪóĆžĚÄ žĄúžßÄÍīÄŽ¶¨ŪĒĄŽ°úÍ∑łŽě®žĚł EndNote X9.2 Ž•ľ žĚīžö©Ūēėžó¨ Í≤ÄŪ܆ŪēėÍ≥† ž†ēŽ¶¨ŪēėžėÄŽč§. PubMedžóźžĄú 69Ūéł, PsycINFOžóźžĄú 58Ūéł, CINAHLžóźžĄú 16ŪéłžúľŽ°ú žīĚ 143ŪéłžĚė ŽÖľŽ¨łžĚī Í≤ÄžÉČŽźėžóąŽč§. žīĚ 143ŪéłžĚė ŽÖľŽ¨ł ž§Ď ž§ĎŽ≥ĶŽźėŽäĒ ŽÖľŽ¨ł 54Ū鳞̥ ž†úÍĪįŪēú Ží§ 89ŪéłžĚė ŽÖľŽ¨łžĚė ž†úŽ™©žĚĄ Í≤ÄŪ܆Ūēú ŪõĄ, 39ŪéłžĚė ŽÖľŽ¨łžĚė žīąŽ°ĚžĚĄ Í≤ÄŪ܆Ūēėžó¨ 9ÍįúžĚė ŽÖľŽ¨łžĚĄ ž†úžôłŪēėžėÄŽč§. Žā®žĚÄ 30ÍįúžĚė Ž¨łŪóĆ ž§Ď žĶúžĘÖž†ĀžúľŽ°ú 22ŪéłžĚė Ž¨łŪóƞ̥ žĄ†ž†ēŪēėžėÄŽč§. ž†úžôłŪēú 8ÍįúžĚė ŽÖľŽ¨łžĚÄ ÍĪīÍįēŪēú žßώ讎ßƞ̥ ŽĆÄžÉĀžúľŽ°ú žóįÍĶ¨ŪĖąŽćė ŽÖľŽ¨łžĚī 4Ūéł, žė•žčúŪ܆žč†žĚĄ Ūą¨žó¨ŪēėžßÄ žēäžĚÄ ŽÖľŽ¨łžĚī 1Ūéł, žöĒžēĹ ŪėēŪÉúžĚė ŽÖľŽ¨łžĚī 1Ūéł, žóįÍĶ¨ ŪĒĄŽ°úŪ܆žĹúŽßĆ ž†úžčúŪēú ŽÖľŽ¨łžĚī 1Ūéł, ŽÖľŪŹČ ŪėēŪÉúžĚė ŽÖľŽ¨łžĚī 1Ūéł žěąžóąŽč§(Figure 1).
4) žěźŽ£Ć ž∂Ēž∂ú ŽįŹ Ž∂ĄžĄĚ
2Ž™ÖžĚė ŽŹÖŽ¶ĹŽźú žóįÍĶ¨žěźÍįÄ žĶúžĘÖ žĄ†ž†ēŽźú 22ŪéłžĚė Ž¨łŪóƞ̥ žĚĹÍ≥† žěźŽ£Ćž∂Ēž∂ú žĖĎžčĚžóź ŽĒįŽĚľ Žāīžö©žĚĄ ž†ēŽ¶¨ŪēėžėÄŽč§. žěźŽ£Ćž∂Ēž∂ú žĖĎžčĚžóźŽäĒ ž†Äžěź, ÍĶ≠ÍįÄ, žč§Ūóė ŽĒĒžěźžĚł, ŽĆÄžÉĀžěź žąėžôÄ žĄĪŽ≥Ą, ŽāėžĚī, Ūą¨žó¨Ūēú žė•žčúŪ܆žč† žö©ŽüČ, ŪĒĆŽĚľžčúŽ≥ī žĘÖŽ•ėžôÄ žö©ŽüČ, ŽĆÄž°įÍĶįžĚė žĘÖŽ•ėžôÄ žąėŽ•ľ ŪŹ¨Ūē®ŪēėžėÄŽč§. ŽėźŪēú, žė•žčúŪ܆žč† Ūą¨žó¨ Ūö®Í≥ľŽ•ľ ŪŹČÍįÄŪēėÍłį žúĄŪēī žč§Ūóėžįłžó¨žěźžóźÍ≤Ć Ž∂ÄÍ≥ľŽźú žąėŪĖČ Í≥ľž†ú(task)ÍįÄ žěąŽäĒ Í≤Ĺžöį Í∑ł Žāīžö©žĚĄ ÍłįŽ°ĚŪēėžėÄŽč§. Í≤įÍ≥ľŪŹČÍįÄ žł°ž†ēÍłįž§ÄžĚÄ žā¨ŪöĆŪĖČŽŹôžßÄŪĎú(CAPS-5, PCL-5, RSDI ŽďĪ), žÉĚŽ¨ľŪĎúžßÄžěź(biomarker)žßÄŪĎú(žĹĒŽ•īŪčįžÜĒ, žė•žčúŪ܆žč† ŽďĪ), žč†Í≤ĹžėĀžÉĀžßÄŪĎú(fmri)Ž°ú ÍĶ¨Ž∂ĄŪēėžó¨ Í≤įÍ≥ľŽ•ľ Ž∂ĄžĄĚŪēėžėÄŽč§.
Í∑ł ž§Ď ž£ľŽ°ú žā¨žö©Žźú žā¨ŪöĆŪĖČŽŹôžßÄŪĎúžóźŽäĒ CAPS-5, PCL-5, RSDI ŽďĪžĚī žěąŽč§. DSM žßĄŽč®Íłįž§Äžóź ÍłįŽįėŪēú CAPSŽäĒ ž¶ĚžÉĀžĚĄ žīĚ 5ÍįÄžßÄ ÍĶįžßĎžúľŽ°ú Ž∂ĄŽ•ėŪēėžó¨ žł°ž†ēŪēėÍ≥†, Ūē©žāįŪēėžó¨ ž¶ĚžÉĀžĚė žč¨ÍįĀŽŹĄŽ•ľ ŪŹČÍįÄŪēėŽäĒŽćį, žīĚž†źžĚĄ Íłįž§ÄžúľŽ°ú 20ž†ź Žč®žúĄŽ°ú ž¶ĚžÉĀžĚė žč¨ÍįĀŽŹĄŽ•ľ Ž∂ĄŽ•ėŪēėžó¨ ž¶ĚžÉĀ ÍĪįžĚė žóÜžĚĆ/Í≤Ĺž¶Ě/žó≠žĻė žĚīŪēė/ž§ĎÍįĄ ž†ēŽŹĄ/ž§Ďž¶ĚžúľŽ°ú Ž∂ĄŽ•ėŪēúŽč§[36]. Weathers ŽďĪ(2013)žóź žĚėŪēī ÍįúŽįúŽźú PCL-5ŽäĒ 20Ž¨łŪē≠žúľŽ°ú ÍĶ¨žĄĪŽźėžóąžúľŽ©į, žßÄŽāú Ūēú Žč¨ÍįĄ Í≤ĹŪóėŪēú ŪôėžěźžĚė ž¶ĚžÉĀ ž†ēŽŹĄŽ•ľ ŪŹČÍįÄŪēúŽč§. PCL-5ŽäĒ PTSDžóź ŽĆÄŪēú Ž≥īž°įžßĄŽč® ŽŹĄÍĶ¨Ž°ú, ž¶ĚžÉĀ ž†źžąėŽ•ľ Ūē©žāįŪēėžó¨ ŪŹČÍįÄŪēėŽäĒŽćį, žīĚž†źžĚÄ 80ž†źžúľŽ°ú žěĄÍ≥ĄžĻėžĚł 31-33ž†ź žĚīžÉĀžúľŽ°ú ŪŹČÍįÄŽźú Í≤ĹžöįžóźŽßĆ žĻėŽ£ĆÍįÄ Ūö®Í≥ľž†ĀžĚł Í≤ÉžúľŽ°ú žēĆŽ†§ž†ł žěąŽč§[37].
5) Ž¨łŪóĆžĚė žßą ŪŹČÍįÄ
Ž¨łŪóĆžĚė žßą ŪŹČÍįÄŽäĒ žĹĒŪĀ¨ŽěÄžĚė ŽĻĄŽö§Ž¶ľ žúĄŪóė ŪŹČÍįÄ ŽŹĄÍĶ¨(Cochrane risk of bias tool)[38]Ž•ľ žā¨žö©Ūēėžó¨, Ž¨īžěĎžúĄ Ž≤ąŪėł žÉĚžĄĪ(random sequence generation), Žįįž†ēžĚÄŽčČ(allocation concealment), žóįÍĶ¨ žįłžó¨žěźžôÄ žóįÍĶ¨žěź ŽßĻÍ≤Ä(blinding of participants and personnel), Í≤įÍ≥ľ ŪŹČÍįÄ ŽßĻÍ≤Ä(blinding of outcome assessment), Ž∂ąž∂©Ž∂ĄŪēú Í≤įÍ≥ľ žěźŽ£Ć(incomplete outcome data), žĄ†ŪÉĚž†Ā Í≤įÍ≥ľ Ž≥īÍ≥†(selective outcome reporting)žôÄ ÍłįŪÉÄ ŪéłŪĖ•(e.g., potential conflict of interest) žó¨Ž∂ÄŽ•ľ ŪŹČÍįÄŪēėžėÄŽč§. ŽĎź Ž™ÖžĚė žóįÍĶ¨žěź ÍįĄžĚė žīąÍłį žĚľžĻėŽŹĄŽäĒ 93% žėÄžúľŽ©į, Ž∂ąžĚľžĻėŪēėŽäĒ Í≤Ĺžöį ž†ú3žĚė žóįÍĶ¨žěźžôÄ ŪöĆžĚėŽ•ľ ŪÜĶŪēīžĄú Ūē©žĻėŪēėžėÄŽč§.
žóįÍĶ¨ Í≤įÍ≥ľ
1. Í≤Ćžě¨ ŽÖľŽ¨łžĚė ŪäĻžĄĪ
ŪŹ¨Ūē®Žźú 22ŪéłžĚė Ž™®Žď† ŽÖľŽ¨łžóźžĄú žė•žčúŪ܆žč†žĚĄ ŽĻĄÍįē žä§ŪĒĄŽ†ąžĚī(Nasal spray)Ž°ú Ūą¨žó¨ŪēėžėÄžúľŽ©į, 22ŪéłžĚė ŽÖľŽ¨ł ž§Ď Žč§ŪöĆ Ūą¨žó¨Ž•ľ žčúŪĖČŪēú 5ŪéłžĚė ŽÖľŽ¨łžóźžĄúŽäĒ 40 IUŽ•ľ žā¨žö©ŪēėžėÄŽč§. 17ÍįúŽäĒ žĚľŪöĆŪą¨žó¨Ž°ú 20 IU (3Ūéł) or 24 IU (6Ūéł) or 40 IU (8Ūéł)Ž•ľ Ūą¨žó¨ŪēėžėÄÍ≥†, 20 IUŽßƞ̥ žā¨žö©Ūēú žóįÍĶ¨ÍįÄ 6Ūéł, 40 IUŽßƞ̥ žā¨žö©Ūēú žóįÍĶ¨ÍįÄ 8ŪéłžĚīžóąŽč§. ŽėźŪēú 10ŪéłžĚė ŽÖľŽ¨łžĚī ŽĄ§ŽćúŽěÄŽďúžóźžĄú, 8ŪéłžĚī ŽĮłÍĶ≠žóźžĄú, 3ŪéłžĚī žĚīžä§ŽĚľžóėžóźžĄú žĚīŽ£®žĖīž°ĆÍ≥†, ŽŹÖžĚľžóźžĄú 1ŪéłžĚė žóįÍĶ¨ÍįÄ žĚīŽ£®žĖīž°ĆŽč§. žóįÍĶ¨ ŽĒĒžěźžĚłžĚÄ ŪĒľŪóėžěź ÍįĄ žĄ§Í≥Ą(between subject design, BS) ŪėĻžĚÄ ŪĒľŪóėžěź Žāī žĄ§Í≥Ą(within subject design, WS)Ž°ú Ž∂ĄŽ•ėŪēėžėÄŽč§. ŪĒľŪóėžěź ÍįĄ žĄ§Í≥Ą žóįÍĶ¨ ŽĒĒžěźžĚłžĚĄ žā¨žö©Ūēú ŽÖľŽ¨łžĚī 9Ūéł, ŪĒľŪóėžěźŽāī žĄ§Í≥Ą žóįÍĶ¨ ŽĒĒžěźžĚłžĚĄ žā¨žö©Ūēú ŽÖľŽ¨łžĚī 13ŪéłžĚīžóąŽč§(Table 1).
Table 1.
Characteristics of Included Studies
| First author (yr) | Country | Design | N randomized (OT, placebo) | N male (%) | Mean age | INOT Administration | Placebo | Control group |
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| Single administration | ||||||||
| Pitman et al. (1993) [A1] | USA | BS | 43 (15, 15) | 43 (100.0 ) | 44.2 | 20 IU, 1 hr before OA | Placebo (saline) in 2-mL solution (same used for INOT) | - |
| Eidelman et al. (2015) [A2] | Israel | WS | 28 (28, 28) | 28 (100.0) | 27.0 | 24 IU, 45 min before OA | Placebo, custom-designed to match drug minus OT | 15 trauma-unexposed |
| Palgi et al. (2016)† [A3] | Israel | WS | 32 (32, 32) | 23 (72.0) | 43.4 | 24 IU, 45 min before OA | Same saline solution where OT was dissolved but without the drug itself. Placebo, not specified. | 30 matched healthy controls |
| Frijling et al. (2016a) [A4] | Netherlands | BS | 44 (24, 20) | 18 (41.0) | 30.8 | 40 IU, 45 min before OA | 0.8% NaCl solution | - |
| Frijling et al. (2016b) [A5] | Netherlands | BS | 41 (23, 18) | 17 (41.4) | 36.0 | 40 IU, 45 min before OA | 0.8% NaCl solution | - |
| Koch et al. (2016a)†† [A6] | Netherlands | WS | 37 (37, 37) | 21 (56.8) | 40.2 | 40 IU, 45 min before OA | Saline, NaCl 0.9% | 40 police officers without PTSD |
| Koch et al. (2016b)§ [A7] | Netherlands | WS | 37 (37, 37) | 21 (56.8) | 40.2 | 40 IU, 45 min before OA | Saline, NaCl 0.9% | 40 police officers without PTSD |
| Nawijn et al. (2016)§ [A8] | Netherlands | WS | 40 (40, 40) | 21 (52.5) | 40.7 | 40 IU, 50-70 min before OA | Saline, NaCl 0.9% | 37 trauma-exposed |
| Palgi et al. (2017)¶ [A9] | Israel | WS | 32 (32, 32) | 23 (72.0) | 43.4 | 24 IU, 45 min before OA | Placebo, not specified | 30 matched healthy controls |
| Sack et al. (2017) [A10] | Germany | WS | 35 (35, 35) | 0 (0.0) | 39.8 | 24 IU, 45 min before OA | Same ingredients as the INOT spray except OT | 10 healthy female controls |
| Nawijn et al. (2017)# [A11] | Netherlands | WS | 40 (40, 40) | 21 (52.5) | 40.7 | 40 IU, 50-70 min before OA | Saline, NaCl 0.8% | 37 trauma-exposed |
| Flanagan et al. (2018a) [A12] | USA | WS | 17 (17, 17) | 9 (52.9) | 36.3 | 24 IU, 45 min before OA | Saline, not specified | 16 childhood trauma exposed |
| Flanagan et al. (2019a) [A13] | USA | WS | 33 (33, 33) | 15 (45.5) | 37.8 | 24 IU, 45 min before OA | Saline | 16 childhood trauma exposed |
| Flanagan et al. (2019b) [A14] | USA | BS | 67 (32, 35) | 67 (100.0) | 49.0 | 40 IU, 45 min before OA | Saline | - |
| Koch et al. (2019) [A15] | Netherlands | WS | 37 (37, 37) | 21 (56.0) | 40.2 | 40 IU, 80 min before OA | Saline, NaCl 0.9% | 40 police officers without PTSD |
| Stauffer et al. (2019) [A16] | USA | WS | 47 (47, 47) | 47 (100.0) | 50.6 | 20 or 40 IU, 30 min before OA | Placebo, not specified | - |
| Morrison et al. (2020) [A17] | USA | WS | 97 (97, 97) | 97 (100.0) | 49.6 | 20 or 40 IU or placebo each week, for 3 weeks, each done 135 min before OA | Placebo, not specified | 43 healthy male |
| Multiple administration | ||||||||
| Zuiden et al. (2017) [A18] | Netherlands | BS | 107 (53, 54) | 54 (50.5) | 35.5 | Assess CAPS at baseline (within 10 days posttrauma) 40 IU BID (80 IU/ day) for 8 days, OA at 1.5, 3, and 6 months posttrauma | Saline, NaCl 0.9% | 54 adults with moderate to severe acute distress |
| Flanagan et al. (2018b) [A19] | USA | BS | 17 (8, 7) | 14 (82.3) | 43.8 | 40 IU each week, for 8 weeks, each done 45 min before OA | Placebo, not specified. | 18 trauma-exposed |
| Engel et al. (2020) [A20] | Netherlands | BS | 100 (49, 51) | 54 (54.0) | 34.2 | Assess CAPS at baseline (within 10 days posttrauma) 40 IU BID (80 IU/ day) for 7 days, OA at 1.5, 3, and 6 months posttrauma | Placebo, not specified | 27 women using hormonal conception, 19 naturally cycling women |
| Flanagan et al. (2020) [A21] | USA | BS | 188 (94, 94) | Not specified | Not specified | Assess CAPS at baseline, 40 IU each week, for 10 weeks, each done 30 min before PE session, OA at week 5, 10, and at 3, 6 months follow-up | Saline | 94 veterans with PTSD |
| Sippel et al. (2020) [A22] | Netherlands | BS | 13 (6, 7) | 10 (76.9) | 42.8 | Assess CAPS at baseline 40 IU each week, for 8 weeks (PE session 2 to 9), Each done 45 min before PE session, OA at session 10 | Placebo, not specified | 7 PTSD patients with placebo |
2. žóįÍĶ¨ ŽĆÄžÉĀžěźžĚė ŪäĻžĄĪÍ≥ľ žė•žčúŪ܆žč† Ūą¨žó¨ Žį©Ž≤ē
ŽĆÄžÉĀžěźŽäĒ žĄĪžĚł(ŽßĆ 18žĄł žĚīžÉĀ)žúľŽ°ú, žóįÍĶ¨ ŽĆÄžÉĀžěźžĚė ŪŹČÍ∑† žóįŽ†ĻŽĆÄŽ•ľ Íłįž§ÄžúľŽ°ú Ž≥īžēėžĚĄ ŽēĆ, 20ŽĆÄžóź ŽĆÄŪēú ŽÖľŽ¨łžĚī 1Ūéł, 30ŽĆÄÍįÄ 7Ūéł, 40ŽĆÄÍįÄ 12Ūéł, 50ŽĆÄÍįÄ 1Ūéł, ŪôēžĚł Ž∂ąÍįÄŪēú ŽÖľŽ¨łžĚī 1ŪéłžĚīžóąŽč§. Žā®žĄĪŽßƞ̥ ŽĆÄžÉĀžúľŽ°ú Ūēú ŽÖľŽ¨łžĚī 5ŪéłžĚīžóąÍ≥†, žó¨žĄĪŽßƞ̥ ŽĆÄžÉĀžúľŽ°ú Ūēú ŽÖľŽ¨łžĚÄ 1ŪéłžĚīžóąŽč§. žóįÍĶ¨ ŽĆÄžÉĀžěź žąėŽäĒ 17-188Ž™Ö žā¨žĚīžėÄÍ≥†, Žā®ŽÖÄ Ž™®ŽĎźŽ•ľ ŪŹ¨Ūē®Ūēú ŽÖľŽ¨łžóźžĄúžĚė Žā®žĄĪžĚė ŽĻĄžú®žĚÄ ž†Ąž≤īž†ĀžúľŽ°ú 41-82.3%žėÄŽč§. ŽėźŪēú Žč§ŪöĆ Ūą¨žó¨Ž•ľ žčúŽŹĄŪēú žóįÍĶ¨ ž§ĎžóźžĄúŽäĒ 40 IUžĒ© ŪēėŽ£®žóź ŽĎź Ž≤ą, 7žĚľ ŪėĻžĚÄ 8žĚľ ŽŹôžēą Ūą¨žó¨Ūēú ŽÖľŽ¨łžĚī 2Ūéł žěąžóąŽč§. 40 IUŽ•ľ Žß§ž£ľ Ūą¨žó¨ŪēėŽ©īžĄú žīĚ 8ž£ľ ŽŹôžēą žßĄŪĖČŪēú ŽÖľŽ¨łžĚī 2Ūéł, 10ž£ľ ŽŹôžēą žßĄŪĖČŪēú ŽÖľŽ¨łžĚī 1ŪéłžĚīžóąŽč§. Žč§ŪöĆ Ūą¨žó¨ ŽÖľŽ¨ł ž§Ď 2Ū鳞󟞥úŽäĒ žßÄžÜćŽÖłž∂úžĻėŽ£Ć(Prolonged exposure therapy, PE)žôÄ Ž≥ĎŪĖČŪēėžó¨ žė•žčúŪ܆žč†žĚė Ūö®Í≥ľŽ•ľ žł°ž†ēŪēėžėÄÍ≥† žôłžÉĀ ŪõĄ žä§Ū䳎†ąžä§ žě•žē† ž≤ôŽŹĄ(Clinician administered PTSD scale, CAPS)Ž•ľ žā¨žö©Ūēėžó¨ ž¶ĚžÉĀ žôĄŪôĒŽ•ľ ŪŹČÍįÄŪēėžėÄŽč§.
3. žė•žčúŪ܆žč†žĚė žĻėŽ£Ćž†Ā Ūö®Í≥ľ ŪŹČÍįÄ žł°ž†ē Žį©Ž≤ēÍ≥ľ Í≤įÍ≥ľ
22ŪéłžĚė žóįÍĶ¨ŽäĒ Í≥ĶŪÜĶž†ĀžúľŽ°ú PTSD ž¶ĚžÉĀžĚė žôĄŪôĒŽ•ľ Ž™©ž†ĀžúľŽ°ú žßĄŪĖČŽźėžóąŽč§(Table 2). ÍĶ¨ž≤īž†ĀžúľŽ°úŽäĒ, Ž∂Äž°ĪŪēú Íįźž†ē ž°įž†ą Žä•Ž†• ÍįúžĄ†Í≥ľ ÍīÄŽ†®Žźú ŽÖľŽ¨łžĚī 11Ūéł, žĄ§Ž¨łžßÄŽ•ľ ŪÜĶŪēī ž¶ĚžÉĀ žč¨ÍįĀŽŹĄ ÍįúžĄ†žĚĄ ŪŹČÍįÄŪēú ŽÖľŽ¨łžĚī 6Ūéł, žÜźžÉĀŽźú Ž≥īžÉĀŪöĆŽ°ú ŽįėžĚĎžĄĪžĚĄ ŪôēžĚłŪēėŽ†§Í≥† ŪĖąŽćė ŽÖľŽ¨łžĚī 2Ūéł, ŽŹôŽįėŽźú žēĆžĹĒžė¨ žā¨žö© žě•žē† ž¶ĚžÉĀ ÍįúžĄ† ž†ēŽŹĄŽ•ľ Ž≥īÍĪįŽāė žā¨ŪöĆž†Ā žä§Ū䳎†ąžä§, žĹĒŽ•īŪčįžÜĒ(cortisol) ŽÜ掏ĄŽ•ľ ÍīÄžįįŪēėÍĪįŽāė, ŽáĆ ŪôúŽŹôžĚė Ž≥ÄŽŹôžĄĪžĚĄ žł°ž†ēŪĖąŽćė žóįÍĶ¨ÍįÄ ÍįĀÍįĀ 1ŪéłžĒ© žěąžóąŽč§.
Table 2.
Purpose and Parameters with Tasks of Included Studies
| Author (yr) | Purpose | Task | Parameters | ||
|---|---|---|---|---|---|
|
|
|||||
| Socio behavioral measures | Neuronal Imaging | Biomarkers | |||
|
|
|||||
| Single administration | |||||
| Pitman et al. (1993) [A1] | The effects of vasopressin and OT on human emotional memory | 2 min mental arithmetic task | Heart rate (BPM), Skin conductance (őľS), Left lateral frontalis electromyographic (őľV) | ||
| Eidelman et al. (2015) [A2] | The effects of OT on spontaneous brain oscillatory activity | No task | Spontaneous brain activity of two dlPFC regions | ||
| Palgi et al. (2016) [A3] | The effects of OT on the capacity for compassion among patients with PTSD and among healthy control (HC) participants | Compassion task | Compassion Biological Motion Task First-and Second-Order ToM (Yoni Task, Cognitive Empathy) | ||
| Frijling et al. (2016a) [A4] | The effects of a single OT administration on resting-state functional connectivity of amygdala-centered emotion regulation and salience networks in recently trauma-exposed individuals with moderate-to-severe acute distress | Face-matching task | Resting-state functional connectivity | ||
| Frijling et al. (2016b) [A5] | The effects of OT on amygdala reactivity to happy, neutral, and fearful faces in recently trauma-exposed individuals | Face-matching task | Amygdala reactivity | ||
| Koch et al. (2016a) [A6] | The effects of a single intranasal OT administration on subjective anxiety and functional connectivity of BLA and CeM amygdala subregions with prefrontal areas (vmPFC) and salience processing areas (insula and dACC) | Face-matching task | Anxiety, nervousness, happiness, and sadness visual analog scales (VAS, 0-100) | CeM, BLA Amygdala functional connectivity | |
| Koch et al. (2016b) [A7] | The effects of OT on amygdala reactivity towards emotional faces in trauma-exposed police officers with and without PTSD | Face-matching task | Bilateral amygdala reactivity | ||
| Nawijn et al. (2016) [A8] | The effects of OT administration on neural motivational processing during monetary reward and loss anticipation in trauma-exposed police officers with and without PTSD, using a monetary incentive delay (MID) task | A monetary incentive delay (MID) task | Reward pathway reactivity | ||
| Palgi et al. (2017) [A9] | Explore empathic deficits in PTSD and to characterize the association between such deficits and the severity of PTSD symptoms | Biological Motion Task |
Emotional Empathy (anger, disgust, fear, happiness, sadness) Cognitive Empathy (ToM task) |
||
| Sack et al. (2017) [A10] | The effects of OT on provoked PTSD symptoms in female PTSD patients | The trauma script challenge | Provoked PTSD symptoms (RSDI questionnaire) | ||
| Nawijn et al. (2017) [A11] | The effects of OT to enhance neural sensitivity to social reward and potentially decrease sensitivity to social punishment in PTSD patients | The social incentive delay (SID) task | Neural responses to social reward and punishment | ||
| Flanagan et al. (2018a) [A12] | The effects of OT on amygdala reactivity to negative emotional cues between individuals with PTSD resulting from childhood trauma versus individuals who had childhood trauma exposure but did not develop PTSD | N-back task | Working memory performance | Left DLPFC-anterior cingulate connectivity | |
| Flanagan et al. (2019a) [A13] | The effects of OT versus placebo on amygdala reactivity to fearful faces among childhood-trauma exposed individuals with PTSD and without PTSD | Facial affect recognition task | Left and right amygdala responses reactivity | ||
| Flanagan et al. (2019b) [A14] | The effects of OT versus placebo on social stress and associated cortisol reactivity among Veterans with co-occurring PTSD and AUD | No task | Salivary cortisol reactivity | ||
| Koch et al. (2019) [A15] | The effects(behavioral and neural) of OT on distraction as emotion regulation strategy in male and female police officers with and without PTSD | The distraction task | Left thalamus activity, Right striatal activity | ||
| Stauffer et al. (2019) [A16] | The effects of OT versus placebo in reducing cue-induced alcohol craving and HR response in male patients with comorbid AUD and PTSD | Cue-induced craving task | Self-Reported Craving | ||
| Morrison et al. (2020) [A17] | The effects of OT on HC and on people with comorbid posttraumatic stress disorder and alcohol use disorder | The imitation-inhibition task | Automatic imitation/congruency effect | ||
| Multiple administration | |||||
| Zuiden et al. (2017) [A18] | The effects of repeated OT administration on clinician-rated PTSD symptom severity at 1.5 months posttrauma | No task | Clinician-Rated PTSD Symptoms (CAPS) | ||
| Flanagan et al. (2018b) [A19] | Examine the feasibility, safety, and preliminary efficacy of augmenting PE with OT | No task | CAPS for DSM-5, PTSD checklist for DSM-5, Beck-depression inventory, Helping alliance questionnaire, Client satisfaction | ||
| Engel et al. (2020) [A20] | The effects of early (posttraumatic) autonomic and endocrine markers on PTSD symptom development | No task |
Autonomic and endocrine markers (1) Heart rate (variability) (2) Saliva resting cortisol, morning (3) Saliva cortisol (4) Saliva cortisol awakening response (CAR) (5) Cortisol suppression by dexamethasone (6) Blood resting oxytocin |
||
| Flanagan et al. (2020) [A21] | The effect of OT administration combined with PE therapy to (1) Reduce PTSD symptom severity, (2) Accelerate the rate of PTSD symptom improvement, and (3) Improve PE adherence and retention rates | No task | CAPS-5, PCL -5 | ||
| Sippel et al. (2020) [A22] | Associations between PTSD symptom severity and peripheral OT levels measured in plasma before and after a course of prolonged exposure (PE) for PTSD | No task |
PTSD symptom severity (1) CAPS-5 (2) PCL -5 |
Peripheral oxytocin level | |
OT=oxytocin; PTSD=post-traumatic stress disorder; PBO=placebo; PFC=prefrontal cortex; vmPFC=ventromedial PFC; DSM=Diagnostic and Statistical Manual of Mental Disorder; dACC=dorsal anterior cingulate cortex; CeM=central medial amygdala; BLA=basolateral; dlPFC=dorsolateral PFC, RSDI=Responses to Scrip-Driven Imagery Scale; AUD=Alcohol Use Disorder; PCL=PTSD checklist.
ž¶ĚžÉĀ ÍįúžĄ†žĚĄ ŪôēžĚłŪēėÍłį žúĄŪēī 15ÍįúžĚė ŽÖľŽ¨łžóźžĄúŽäĒ žąėŪĖČ Í≥ľž†úŽ•ľ žč§žčú Ūēėžó¨ ŪŹČÍįÄŪĖąžßÄŽßĆ 7ŪéłžĚú ŽÖľŽ¨łžóźžĄúŽäĒ žąėŪĖČ Í≥ľž†úŽ•ľ žč§žčúŪēėžßÄ žēäžēėŽč§. 5ŪéłžĚė žóįÍĶ¨žóźžĄú žĖľÍĶī Žßěž∂ĒÍłį Í≥ľž†ú(face-matching task)Ž•ľ žč§žčúŪēėžó¨ žė•žčúŪ܆žč†žĚī Ž∂Äž†ēž†ĀžĚł Íįźž†ēž†Ā ŽįėžĚϞ̥ ÍįźžÜĆžčúŪā§ŽäĒžßÄ ŪôēžĚłŪēėžėÄÍ≥†, žė•žčúŪ܆žč† Ūą¨žó¨ ŪõĄ Ž≥īžÉĀ(reward)Íłįž†ĄžĚė ŽįėžĚĎžĄĪžĚĄ ŪôēžĚłŪēėÍĪįŽāė, ÍłįžĖĶŽ†•(memory) ŪĖ•žÉĀ ž†ēŽŹĄŽ•ľ ŪĆĆžēÖŪēėÍłį žúĄŪēú Í≥ľž†úŽ•ľ žčúŪĖČŪēėžėÄŽč§.
22ŪéłžĚė ŽÖľŽ¨łžóźžĄú žĚīžö©Ūēú žė•žčúŪ܆žč†žĚė Ūö®Í≥ľžĄĪ ŪŹČÍįÄ ŽŹĄÍĶ¨(parameter)ŽäĒ žā¨ŪöĆ ŪĖČŽŹô žł°ž†ē(Socio-behavioral measure) 11Ūéł, žč†Í≤Ĺ žėĀžÉĀ(Neuronal imaging) 9Ūéł, žÉĚŽ¨ľŪĎúžßÄžěź(Biomarkers) 4ŪéłžúľŽ°ú ŪôēžĚłŽźėžóąŽč§. žā¨ŪöĆ ŪĖČŽŹôžĚė Ž≥ÄŪôĒŽ•ľ ÍīÄžįįŪēú ŽÖľŽ¨łžóźžĄúŽäĒ ž£ľŽ°ú žĄ§Ž¨łžßÄŽ•ľ žā¨žö©ŪĖąŽäĒŽćį Clinician-Administered PTSD Scale for DSM-5 (CAPS-5), PTSD checklist for DSM-5 (PCL-5), responses to script-driven imagery scale (RSDI)Ž•ľ žā¨žö©ŪĖąŽč§. žč†Í≤Ĺ žėĀžÉĀžĚĄ ŪÜĶŪēī ŪŹČÍįÄŪēú ŽÖľŽ¨ł 9ŪéłžĚÄ Ž™®ŽĎź ÍłįŽä•ž†Ā žěźÍłįÍ≥ĶŽ™Ö žėĀžÉĀ(functional magnetic resonance imaging, fMRI)žĚĄ žā¨žö©ŪĖąŽč§. žÉĚŽ¨ľ ŪĎúžßĞ쟎•ľ ŪŹČÍįÄ ŽŹĄÍĶ¨Ž°ú žĚīžö©Ūēú ŽÖľŽ¨łžóźžĄúŽäĒ žěźžú®žč†Í≤ĹÍ≥Ą ŪėĻžĚÄ ŽāīŽ∂ĄŽĻĄÍ≥Ą žßÄŪĎúŽ•ľ žĚīžö©ŪĖąŽč§(Table 3).
Table 3.
Outcome of Included Studies / fMRI / Biomarker / Social behavior
| Author (yr) | Parameters | Outcome |
|---|---|---|
|
|
||
| Socio behavioral measures | ||
| Koch et al. (2016a) [A6] | Anxiety, Nervousness, Happiness, and Sadness visual analog scales (VAS, 0-100) | OT: Subjective anxiety‚Üď; Nervousness‚Üď |
| Palgi et al. (2016) [A3] |
Compassion Biological motion task First- and Second-order ToM (Yoni Task, Cognitive Empathy) |
PBO: Compassion score‚Üď OT (F): Compassion score‚ÜĎ |
| Palgi et al. (2017) [A9] | Emotional empathy (Anger, Disgust, Fear, Happiness, Sadness) | |
| Cognitive empathy (ToM task) | No main effects were found | |
| Sack et al. (2017) [A10] | Provoked PTSD symptoms (RSDI questionnaire) | OT: PTSD symptoms‚Üď |
| Flanagan et al. (2018a) [A12] | Working memory performance |
PBO: Working memory performance‚Üď OT: Working memory performance (-) |
| Stauffer et al. (2019) [A16] | Self-reported craving | No main effect were found |
| Morrison et al. (2020) [A17] | Automatic imitation | OT: Log CE‚ÜĎ |
| Zuiden et al. (2017)‚Ć [A18] | Clinician-rated PTSD symptoms (CAPS) | OT: CAPS scores‚Üď |
| Flanagan et al. (2018b)‚Ć [A19] | CAPS for DSM-5, PTSD checklist for DSM-5, BDI, Helping alliance questionnaire, Client satisfaction, | OT: PCL-5 score marginally‚Üďat end of treatment |
| Flanagan et al. (2020)‚Ć [A21] | CAPS-5, PCL-5 | OT: CAPS-5 scores‚Üď; PCL-5 scores‚Üďfollowing 10 weeks of treatment |
| Sippel et al. (2020)‚Ć [A22] | PTSD symptom severity | OT: PCL-5 score marginally‚Üďat end of treatment |
| (1) CAPS-5 | PCL-5 score significantly‚Üďat session 3 | |
| (2) PCL-5 | ||
| Biomarkers | ||
| Pitman et al. (1993) [A1] | Heart rate (BPM), Skin conductance (őľS), left lateral frontalis electromyographic (őľV) | (Linear contrasts: vasopression>Pitressin>Oxytocin) |
| OT: Heart rate (BPM): F (1,40)<1 | ||
| Skin conductance (őľS): F (1,40)=3.7, p=.06 | ||
| Left lateral frontalis electromyographic (őľV): F (1,40)=10.4, p=.003 | ||
| Flanagan et al. (2019b) [A14] | Salivary cortisol reactivity | OT: cortisol reactivity‚Üď |
| Engel et al. (2020)† [A20] | Autonomic and endocrine markers | OT (F): Higher oxytocin concentrations were associated with higher PTSD symptoms |
|
(1) Heart rate (variability) (2) Saliva resting cortisol, morning (3) Saliva cortisol (4) Saliva cortisol awakening response (CAR) (5) Cortisol suppression by dexamethasone (6) Blood resting oxytocin |
||
| Sippel et al. (2020)† [A22] | Peripheral oxytocin level | No main effects were found |
| Neuronal Imaging | ||
| Eidelman et al. (2015) [A2] | Spontaneous brain activity of two dlPFC regions |
HC: Left dorsolateral prefrontal cortex (dlPFC), Superior frontal gyrus (SFG), the middle frontal gyrus (MFG) reactivity‚ÜĎ OT: Left dorsolateral prefrontal cortex (dlPFC), Superior frontal gyrus (SFG), the middle frontal gyrus (MFG) reactivity (-) |
| Frijling et al. (2016a) [A4] | Resting-state functional connectivity |
OT: Amygdala-insula connectivity‚ÜĎ, Amygdala-vmPFC connectivity‚Üď PBO: Amygdala-vmPFC connectivity‚ÜĎ |
| Frijling et al. (2016b) [A5] | Amygdala reactivity |
OT: Right Amygdala reactivity‚ÜĎ OT (F): Left Amygdala reactivity‚ÜĎ |
| Koch et al. (2016a) [A6] | CeM, BLA Amygdala functional connectivity |
OT (M): Right CeM-left vmPFC‚ÜĎ PBO (M): Right CeM-left vmPFC‚Üď OT (F): Right BLA-right dACC‚Üď OT (F): Right BLA-left dACC‚Üď HC OT (M): Right BLA-left dACC‚Üď |
| Koch et al. (2016b) [A7] | Bilateral amygdala reactivity |
OT: Left Amygdala reactivity‚Üď HC OT: Left Amygdala reactivity‚ÜĎ |
| Nawijn et al. (2016) [A8] | Reward pathway reactivity | OT: Striatum (putamen), Right dACC, right insula‚ÜĎ |
| Nawijn et al. (2017) [A11] | Neural responses to social reward and punishment |
PBO: Left anterior insula‚Üď OT: Left anterior insula (-), Right putamen‚ÜĎ |
| Flanagan et al. (2018a) [A12] | Left dlPFC-anterior cingulate connectivity | OT: Left dlPFC-anterior cingulate‚ÜĎ |
| Flanagan et al. (2019a) [A13] | Left and right amygdala responses (reactivity) |
OT, PBO: Right amygdala reactivity‚ÜĎ HC OT: Left amygdala reactivity‚ÜĎ |
| Koch et al. (2019) [A15] | Emotional processing areas (i.e., amygdala and insula), emotional control areas (i.e., thalamus, hippocampus, caudate nucleus, anterior cingulate cortex and medial prefrontal cortex) |
OT: Amygdala-left thalamus‚ÜĎleft thalamus reactivity‚ÜĎ PBO (F): Right amygdala down-regulation‚ÜĎ OT (F): Right amygdala down-regulation (-) |
1) žā¨ŪöĆ ŪĖČŽŹô žßÄŪĎú ŽįŹ žÉĚŽ¨ľŪĎúžßÄžěź žßÄŪĎú Í≤įÍ≥ľ
žā¨ŪöĆ ŪĖČŽŹô žßÄŪĎúŽ•ľ ŪŹČÍįÄŪēėžó¨ PTSD ž¶ĚžÉĀ Ž≥ÄŪôĒ ž†ēŽŹĄžóź žú†žĚėŽĮłŪēú Ž≥ÄŪôĒŽ•ľ ÍīÄžįįŪēú ŽÖľŽ¨łžĚÄ žīĚ 6ŪéłžĚīŽč§. RSDIŽ•ľ žā¨žö©Ūēú ŽÖľŽ¨łžĚī 1Ūéł, CAPS-5Ž•ľ žā¨žö©Ūēú ŽÖľŽ¨łžĚī 3Ūéł, CAPS-5žôÄ ŽŹôžčúžóź PCL-5Ž•ľ žā¨žö©Ūēú ŽÖľŽ¨łžĚī 3ŪéłžĚīžóąŽč§. žė•žčúŪ܆žč† Ūą¨žó¨ ŪõĄ, žĚėŽ£ĆžßĄžĚī PTSD ž¶ĚžÉĀžĚė ž†ēŽŹĄŽ•ľ ŪŹČÍįÄŪēėŽäĒ ‚ÄúCAPS-5‚ÄĚ ž†źžąėÍįÄ ÍįźžÜĆŪēú žóįÍĶ¨ ž§Ď[A21,A18], Flanagan ŽďĪ[A21]žĚė žóįÍĶ¨žóźžĄúŽäĒ, ŽĆÄž°įÍĶįžóź ŽĻĄŪēīžĄú CAPS-5ž†źžąėŽäĒ 67% ÍįźžÜĆŪēėÍ≥†, PCL-5 ž†źžąėŽŹĄ 61% ÍįźžÜĆŪĖąŽč§. RSDI žĄ§Ž¨łžßÄŽ•ľ ŪÜĶŪēī ž¶ĚžÉĀ žôĄŪôĒŽ•ľ ÍīÄžįįŪĖąŽćė žóįÍĶ¨[A10]žôÄ PCL-5Ž•ľ žā¨žö©Ūēú žóįÍĶ¨žóźžĄúŽŹĄ ž†źžąėÍįÄ ÍįźžÜĆŪē®žĚĄ ŪôēžĚłŪē† žąė žěąžóąŽč§[A21,A12,A22]. Sippel ŽďĪ[A22]žĚė žóįÍĶ¨žóźžĄúŽäĒ, žĻėŽ£Ć ž†ĄŪõĄ ž†źžąėŽ•ľ žł°ž†ēŪēú Í≤įÍ≥ľ, ŽĆÄž°įÍĶįžĚė Í≤Ĺžöį CAPS-5 ž†źžąėÍįÄ 37.29ž†źžóźžĄú 17.71ž†źžúľŽ°ú, PCL-5 ž†źžąėÍįÄ 51.00ž†źžóźžĄú 29.71ž†źžúľŽ°ú, žč§ŪóėÍĶįžĚė Í≤Ĺžöį CAPS-5 ž†źžąėÍįÄ 38.00ž†źžóźžĄú 13.0ž†źžúľŽ°ú, PCL-5 ž†źžąėÍįÄ 50.17ž†źžóźžĄú 20.50ž†źžúľŽ°ú ÍįźžÜĆŪĖąŽč§. ŽėźŪēú PTSD ŪôėžěźžĚė žė•žčúŪ܆žč†žúľŽ°ú žĚłŪēú ‚ÄėÍ≥ĶÍįź Žä•Ž†•‚ÄôžĚė Ž≥ÄŪôĒŽ•ľ žóįÍĶ¨Ūēú ŽÖľŽ¨łŽŹĄ žěąžóąŽäĒŽćį, žė•žčúŪ܆žč† Ūą¨žó¨ žĚīŪõĄ ŽŹôž†ēžč¨(compassion)žĚī ŽÜížēĄž°ĆŽč§Í≥† Ž≥īÍ≥†Ūēú žóįÍĶ¨[A9]žôÄ ŪÉĞ̳žĚė Íįźž†ēÍ≥ľ ŪĖČŽŹôžĚĄ Ž™®Žį©Ūē† žąė žěąŽäĒ Žä•Ž†•žĚī ÍįúžĄ†ŽźėžóąŽč§ŽäĒ žóįÍĶ¨ÍįÄ žěąžóąŽč§[A17]. žÉĚŽ¨ľŪĎúžßĞ쟎•ľ žĚīžö©Ūēú ŽÖľŽ¨ł ž§Ď, ŪÉÄžē° žĹĒŽ•īŪčįžÜĒžĚĄ žł°ž†ēŪēú žóįÍĶ¨ÍįÄ 2Ūéł[A20,A14], žēąž†ē žčú Ūėąž§Ď žė•žčúŪ܆žč†žĚīŽāė žĹĒŽ•īŪčįžÜĒžĚĄ žł°ž†ēŪēú žóįÍĶ¨ÍįÄ ÍįĀ ŪēúŪéł žĒ© žěąžóąžúľŽ©į[A22,A20], žč¨Žįēžąė, ŪĒľŽ∂Ä ž†ĄŽŹĄžôÄ Í∑ľž†ĄŽŹĄŽ•ľ ÍīÄžįįŪēú žóįÍĶ¨ÍįÄ Ūēú Ūéł žěąžóąŽč§[A1]. žěźÍ∑ĻžĚĄ ž£ľÍ≥†, žč§ŪóėÍĶįžóźžĄú ŽāģžĚÄ ŽįėžĚĎžĄĪžĚĄ ŪôēžĚłŪēú žóįÍĶ¨ŽŹĄ žěąžóąŽč§[A19].
2) žč†Í≤Ĺ žėĀžÉĀ žßÄŪĎú Í≤įÍ≥ľ(fMRI)
žč†Í≤Ĺ žėĀžÉĀ žßÄŪĎúŽ•ľ Í≤įÍ≥ľŽ°ú žāľžĚÄ 9ŪéłžĚė žóįÍĶ¨ŽäĒ ŪĀ¨Í≤Ć ŽĎź ÍįÄžßÄŽ°ú Ž∂ĄŽ•ėŪē† žąė žěąŽč§. ŪäĻž†ē Í≥ľž†ú(task)ÍįÄ ž£ľžĖīžßĄ ŪõĄ, Ū鳎ŹĄž≤ī(amygdala)Ž•ľ ž§Ďžč¨žúľŽ°ú Ūēėžó¨ ŽáĆžĚė Žč§Ž•ł Ž∂ÄžúĄžôÄžĚė žóįÍ≤įžĄĪ(connectivity)žĚĄ ÍīÄžįįŪēú žóįÍĶ¨žôÄ, ŽáĆžĚė ŪäĻž†ē Ž∂ÄžúĄžĚė ŽįėžĚĎžĄĪ(reactivity) Ž≥ÄŪôĒŽ•ľ ÍīÄžįįŪēú žóįÍĶ¨ÍįÄ žěąŽč§. žóįÍ≤įžĄĪžĚĄ ÍīÄžįįŪēú žóįÍĶ¨ŽäĒ žīĚ 3Ūéł, ŽįėžĚĎžĄĪ Ž≥ÄŪôĒŽ•ľ žł°ž†ēŪēú žóįÍĶ¨ŽäĒ 6ŪéłžĚīŽč§. Í≥ľž†úŽ≥ĄŽ°ú Í≤įÍ≥ľŽ•ľ žāīŪéīŽ≥īžěźŽ©ī, žĖľÍĶī Žßěž∂ĒÍłį Í≥ľž†ú(face-matching task)Ž•ľ žąėŪĖČŪēú žóįÍĶ¨žóźžĄú žė•žčúŪ܆žč†Ūą¨žó¨ ŪõĄ, ŽĆÄŽáĆžĄ¨(insula)Í≥ľ Ū鳎ŹĄž≤ī, Ū鳎ŹĄž≤īžôÄ Ž≥ĶŽ∂Ä ž†ĄŽĎźžóĹ ŪĒľžßą(ventromedial prefrontal cortex, vmPFC)žĚė žóįÍ≤įžĄĪžĚī ÍįēŪôĒŽźėžóąÍ≥†[A4], žė§Ž•łž™Ĺ Ū鳎ŹĄž≤ī žěźž≤īžĚė ŽįėžĚĎžĄĪŽŹĄ ŪôúžĄĪŪôĒŽźėžóąŽč§[A5]. Žėź, Žč§Ž•ł žóįÍĶ¨žóźžĄúŽäĒ žė§Ž•łž™Ĺ ž§Ďžč¨ Žāīžł° Ū鳎ŹĄž≤īžôÄ žôľž™Ĺ Ž≥ĶŽ∂Ä ž†ĄŽĎźžóĹ ŪĒľžßąžĚė žóįÍ≤įžĄĪžĚī žė•žčúŪ܆žč†žĚĄ Ūą¨žó¨Ūēú žĚīŪõĄ Žā®žĄĪ žč§ŪóėÍĶįžóźžĄú ÍįēŪôĒŽźėžóąÍ≥†, žó¨žĄĪ žč§ŪóėÍĶįžóźžĄú žė§Ž•łž™Ĺ Íłįž†Ä žł° Ū鳎ŹĄž≤ī(basolateral amygdala)žôÄ Žįįžł° ž†ĄŽĆÄžÉĀ ŪĒľžßą(dorsal anterior cingulate cortex, dACC)žĚė žóįÍ≤įžĄĪžĚÄ žēĹŪôĒŽźėÍĪįŽāė[A6], žôľž™Ĺ Ū鳎ŹĄž≤īžĚė ŽįėžĚĎžĄĪžĚī ž†ÄŪēėŽźėžóąŽč§[A7]. ÍįôžĚÄ Í≥ľž†úŽ•ľ ž†Āžö©Ūēú Žč§Ž•ł žóįÍĶ¨žóźžĄúŽäĒ žč§ŪóėÍĶįÍ≥ľ ŽĆÄž°įÍĶį Ž™®ŽĎź žė§Ž•łž™Ĺ Ū鳎ŹĄž≤īžĚė ŽįėžĚĎžĄĪžĚī ŽÜížēĄž°ĆŽč§[A6]. žßĎž§Ď Žį©Ūēī Í≥ľž†ú(distraction task)Ž•ľ žąėŪĖČŪēú žóįÍĶ¨žóźžĄúŽäĒ Ū鳎ŹĄž≤īžôÄ žôľž™Ĺ žčúžÉĀžĚė žóįÍ≤įžĄĪžĚī žč§ŪóėÍĶįžóźžĄú ŽÜížēĄž°ĆŽč§[A15]. Ž≥īžÉĀ(reward)žĚĄ ž£ľŽäĒ Í≥ľž†úŽ•ľ žąėŪĖČŪēú žóįÍĶ¨žóźžĄúŽäĒ žĄ†ž°įž≤ī(striatum)žôÄ žöįŽįįžł° ž†ĄŽĆÄžÉĀ ŪĒľžßą(right dorsal anterior cingulate cortex, right dorsal ACC), žė§Ž•łž™Ĺ ŪĒľÍįĀ(putamen)žóźžĄú ŽįėžĚĎžĄĪžĚī ŽÜížēĄž°ĆŽč§[A8,A11]. ÍłįžĖĶ(memory)Í≥ľ ÍīÄŽ†®Žźú Í≥ľž†úŽ•ľ žąėŪĖČŪēú žóįÍĶ¨žóźžĄúŽäĒ žĘĆŽįįžôłžł° ž†Ąž†ĄŽĎź ŪĒľžßą(left dorsolateral prefrontal cortex)Í≥ľ ž†ĄŽį© ŽĆÄžÉĀ(anterior cingulate)žĚė žóįÍ≤įžĄĪžĚī žč§ŪóėÍĶįžóźžĄú ŽÜížēĄž°ĆŽč§[A15].
4. Ž¨łŪóĆžĚė ŪŹČÍįÄ
Ž¨łŪóĆžĚė žßą ŪŹČÍįÄŽäĒ žĹĒŪĀ¨ŽěÄžĚė ŽĻĄŽö§Ž¶ľ žúĄŪóė ŪŹČÍįÄ ŽŹĄÍĶ¨(the Cochrane Collaboration‚Äôs tool for assessing risk of bias in randomized trials)[38]Ž•ľ žĚīžö©Ūēėžó¨ žā¨ž†ēŪēėžėÄÍ≥†, Í∑ł Í≤įÍ≥ľŽäĒ Table 4žóź ž†úžčúŪēėžėÄŽč§. Ž¨īžěĎžúĄ Ž≤ąŪėł žÉĚžĄĪ(Random sequence generation) žó¨Ž∂ÄžôÄ Žįįž†ēžĚÄŽčČ(Allocation concealment) žó¨Ž∂ÄŽäĒ 22ŪéłžĚė ŽÖľŽ¨ł ž§Ďžóź 5Ūéł(22.7%) [A21-A10,A14,A16]žóźžĄúŽßĆ Ž™ÖŪôēŪēėÍ≤Ć ž†úžčúŪēėžėÄÍ≥†, ŽāėŽ®łžßÄ 17ŪéłžĚė ŽÖľŽ¨łžóźžĄúŽäĒ ž∂©Ž∂ĄŪēú ž†ēŽ≥īŽ•ľ ž†úÍ≥ĶŪēėžßÄ žēäžēĄ Ž∂ąŪôēžč§(Uncertain) ŽďĪͳȞúľŽ°ú ŪŹČÍįÄŪēėžėÄŽč§. žóįÍĶ¨ žįłžó¨žěźžôÄ žóįÍĶ¨žěź ŽßĻÍ≤Ä(Blinding of participants and personnel) Ūē≠Ž™©žĚÄ Ž™®Žď† ŽÖľŽ¨łžóźžĄú Ž™ÖŪôēŪěą Íłįžą†ŽźėžĖī žěąžóąŽč§. Í∑łŽü¨Žāė, Í≤įÍ≥ľ ŪŹČÍįÄ ŽßĻÍ≤Ä(Blinding of outcome assessment) Ūē≠Ž™©žĚÄ 8ŪéłžĚė ŽÖľŽ¨ł(36.4%)[A21-A22,A14,A19,A16]žóźžĄúŽßĆ Ž™ÖŪôēŪēėÍ≤Ć ž†úžčúŪēėžėÄÍ≥†, 14ŪéłžĚė ŽÖľŽ¨łžóźžĄúŽäĒ Ž™ÖŪôēŪēėÍ≤Ć ž†úžčúŪēėžßÄ žēäžēĄ Ž∂ąŪôēžč§(Uncertain)žúľŽ°ú ŪŹČÍįÄŪēėžėÄŽč§. Í≤įÍ≥ľ žěźŽ£ĆÍįÄ žôĄž†ĄŪēėžßÄ žēäŽč§Í≥† ŪĆźŽč®ŽźėŽäĒ ŽÖľŽ¨łžĚÄ žóÜžóąžúľŽāė, Í≤įÍ≥ľŽ•ľ žĄ†ŪÉĚž†Ā žúľŽ°ú Ž≥īÍ≥†ŪĖąŽäĒžßÄ žó¨Ž∂ÄŽ•ľ ŪĆźŽč®Ūē† žąė žěąŽäĒ Í∑ľÍĪįŽ•ľ ŽįúÍ≤¨ŪēėžßÄŽäĒ Ž™ĽŪēėžó¨, Ž™®Žď† ŽÖľŽ¨łžóź Ž∂ąŪôēžč§(Uncertain) ŽďĪͳȞ̥ Ž∂Äžó¨ŪēėžėÄŽč§.
Table 4.
Risk of Bias in Included Studies
| Random sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective outcome reporting | Other sources of bias | |
|---|---|---|---|---|---|---|---|
|
|
|||||||
| Single administration | |||||||
| Pitman et al. (1993) [A1] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Eidelman et al. (2015) [A2] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | High |
| Palgi et al. (2016) [A3] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Frijling et al. (2016a) [A4] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Frijling et al. (2016b) [A5] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Koch et al. (2016a) [A6] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Koch et al. (2016b) [A7] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Nawijn et al. (2016) [A8] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Palgi et al. (2017) [A9] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Sack et al. (2017) [A10] | Low | Low | Low | Low | Low | Uncertain | Low |
| Nawijn et al. (2017) [A11] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Flanagan et al. (2018a) [A12] | Uncertain | Uncertain | Low | Low | Low | Uncertain | Low |
| Flanagan et al. (2019a) [A13] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Flanagan et al. (2019b) [A14] | Low | Low | Low | Low | Low | Uncertain | Low |
| Koch et al. (2019) [A15] | Uncertain | Uncertain | Low | Uncertain (Low) | Low | Uncertain | Low |
| Stauffer et al. (2019) [A16] | Low | Low | Low | Low | Low | Uncertain | Low |
| Morrison et al. (2020) [A17] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Multiple administration | |||||||
| Zuiden et al. (2017) [A18] | Low | Low | Low | Low | Low | Uncertain | Low |
| Flanagan et al. (2018b) [A19] | Uncertain | Uncertain | Low | Low | Low | Uncertain | Low |
| Engel et al. (2020) [A20] | Uncertain | Uncertain | Low | Uncertain | Low | Uncertain | Low |
| Flanagan et al. (2020) [A21] | Low | Low | Low | Low | Low | Uncertain | Low |
| Sippel et al. (2020) [A22] | Uncertain | Uncertain | Low | Low | Low | Uncertain | Low |
ŽÖľ žĚė
Ž≥ł žóįÍĶ¨ŽäĒ ž≤īÍ≥Ąž†ĀžĚł Ž¨łŪóĆÍ≥†žįįžĚĄ ŪÜĶŪēī žė•žčúŪ܆žč†žĚė Ūą¨žó¨ž°įÍĪīÍ≥ľ Ūö®Í≥ľ ŪŹČÍįÄžßÄŪĎúŽ•ľ Ž∂ĄžĄĚŪē®žúľŽ°úžć® PTSD žĻėŽ£Ćž†úŽ°úžĄúžĚė žė•žčúŪ܆žč†žĚė ÍįÄŽä•žĄĪžĚĄ ŪôēžĚłŪēėÍ≥†žěź žąėŪĖČŽźėžóąŽč§. žė•žčúŪ܆žč†žĚė PTSD žĻėŽ£Ćž†úŽ°úžĄúžĚė ÍįÄŽä•žĄĪžĚĄ ž≤ėžĚĆžúľŽ°ú ŪŹČÍįÄŪēú Pitman ŽďĪ[A1]žĚė žóįÍĶ¨ŽäĒ Ž≤†Ū䳎ā® žįłž†Ąžö©žā¨Ž•ľ ŽĆÄžÉĀžúľŽ°ú žė•žčúŪ܆žč†žĚĄ Ūą¨žó¨Ūēėžó¨ ž†ĄŪą¨ žĚīŽĮłžßÄžóź ŽĆÄŪēī ŽįėžĚĎžĄĪžĚī ÍįźžÜĆŪēú Í≤įÍ≥ľŽ•ľ ž†úžčúŪēėžó¨ žôłžÉĀžĄĪ ÍłįžĖĶžóź ŽĆÄŪēī žė•žčúŪ܆žč†žĚė žĻėŽ£Ćž†Ā ÍįÄŽä•žĄĪžĚĄ Ž≥īÍ≥†ŪēėžėÄŽč§. ŽėźŪēú ŽŹôŽ¨ľžč§Ūóė Í≤įÍ≥ľŽ•ľ Í∑ľÍĪįŽ°ú 2015ŽÖĄ žĚīŪõĄ, žė•žčúŪ܆žč† 1ŪöĆ Ūą¨žó¨Ž•ľ ŪÜĶŪēī PTSDžóź ŽĆÄŪēú Ūö®Í≥ľŽ•ľ ŪŹČÍįÄŪēėŽ†§ŽäĒ žčúŽŹĄÍįÄ žĚīŽ£®žĖīžßÄÍ≥† žěąžúľŽ©į, Giovanna ŽďĪžĚė ž≤īÍ≥Ąž†Ā Ž¨łŪóĆÍ≥†žįį žóįÍĶ¨[35]žóźžĄúŽäĒ, žóįÍĶ¨ Í≤įÍ≥ľÍįÄ Ž™®ŽĎź žĚľÍīÄŽźėžßÄŽäĒ žēäžßÄŽßĆ, ÍĶźÍįźžč†Í≤ĹÍ≥ĄžôÄ žĹĒŽ•īŪčįžÜĒ ŽįėžĚĎžĄĪ ž°įž†ą, ŪúīžčĚ žÉĀŪÉú ŪėĻžĚÄ ŪäĻž†ē žąėŪĖČ Í≥ľž†úŽ•ľ žąėŪĖČŪēú ŪõĄ žč†Í≤Ĺ žėĀžÉĀ Í≤įÍ≥ľžóźžĄú žė•žčúŪ܆žč† Ūą¨žó¨ÍĶįžĚī ŽĆÄž°įÍĶįÍ≥ľ žį®žĚīŽ•ľ Ž≥īžėÄžĚƞ̥ Ž≥īÍ≥†Ūēėžó¨ žė•žčúŪ܆žč†žĚė PTSD žĻėŽ£Ćž†úŽ°úžĄúžĚė ÍįÄŽä•žĄĪžĚĄ ž≤ėžĚĆžúľŽ°ú ŪôēžĚłŪēėžėÄŽč§[35].
2016ŽÖĄžóź žčúŪĖČŽźú Janezic ŽďĪ[39]žĚė žĄ§žĻėŽ•ėžóź ÍīÄŪēú žóįÍĶ¨žóźžĄú, žč¨ÍįĀŪēú žä§Ū䳎†ąžä§ žöĒžĚł žßĀŪõĄžĚė žė•žčúŪ܆žč†žĚė žĚľŪöĆ ŪĒľŪēė Ūą¨žó¨ÍįÄ ŪõĄžÜć Í≥ĶŪŹ¨ žėĀŪĖ•žóź ŽĮłžĻėžßÄ žēäÍ≥†, 2žĚľ ŪõĄžĚė žä§Ū䳎†ąžä§ žöĒžĚłžóź žě¨ŽÖłž∂ú ŽźėžóąžĚĄ ŽēĆ, žÉĀŪô©Ž≥Ą Í≥ĶŪŹ¨ ÍłįžĖĶžĚĄ ž¶ĚÍįÄžčúžľįžĚƞ̥ ŪôēžĚłŪĖąŽč§. ŪēėžßÄŽßĆ 7žĚľ ŽėźŽäĒ 14žĚľ ŽŹôžēąžĚė ŽįėŽ≥Ķž†ĀžĚīÍ≥† ŽßĆžĄĪž†ĀžĚł ŪĒľŪēė žė•žčúŪ܆žč† Ūą¨žó¨ŽäĒ žä§Ū䳎†ąžä§Ž•ľ Í≤™žĚÄ žßÄ 14žĚľ ŪõĄžóź Í≥ĶŪŹ¨žĚė žĚľŽįėŪôĒŽ•ľ ÍįźžÜĆžčúžľįžĚƞ̥ Ž≥īžėÄŽč§. žĚīŪõĄ, žė•žčúŪ܆žč†žĚė Žč§ŪöĆ Ūą¨žó¨ÍįÄ žĚľŪöĆžĄĪ Ūą¨žó¨žôÄŽäĒ Žč§Ž•ł Žį©žčĚžúľŽ°ú, PTSDžóź ŽĆÄŪēú žěĄžÉĀž†Ā Ūö®Í≥ľŽ•ľ ŽāėŪÉÄŽāľ žąė žěąžĚƞ̥ Ž≥īžĚīÍłį žúĄŪēī žė•žčúŪ܆žč†žĚĄ Žč§ŪöĆ Ūą¨žó¨Ž•ľ žčúŽŹĄŪēėŽäĒ žóįÍĶ¨ÍįÄ ŽďĪžě•ŪēėžėÄŽč§. ŽėźŪēú žč¨Ž¶¨žĻėŽ£Ć ž§Ď ŪēėŽāėžĚł ŽÖłž∂úžĻėŽ£ĆžĚė Ž≥īž°į žĻėŽ£Ćž†úŽ°úžĄúžĚė žė•žčúŪ܆žč†žĚė Ūö®Í≥ľŽ•ľ ŪŹČÍįÄŪēėÍ≤Ć ŽźėžóąŽč§[A21,A22]. ŽÖłž∂úžĻėŽ£ĆŽäĒ ŪôėžěźÍįÄ ŽĎźŽ†§žõĞ̥ žßĀŽ©īŪē† žąė žěąŽŹĄŽ°Ě ŽŹēŽäĒ žĚłžßÄ ŪĖČŽŹôžĻėŽ£ĆžĚė žĚľžĘÖžúľŽ°ú, ŪôėžěźÍįÄ žôłžÉĀ žā¨ÍĪīžóź ŽĆÄŪēī žßĀž†Ď žĚīžēľÍłįŪēėŽ©īžĄú Íįźž†ēžĚĄ žßĀž†Ďž†ĀžúľŽ°ú žßĀŽ©īŪēėŽäĒ žÉĀžÉĀž†Ā ŽÖłž∂ú(Imaginary exposure)ÍłįŽ≤ēžĚĄ žā¨žö©Ūēėžó¨ žôłžÉĀ žā¨ÍĪīžóź ŽĆÄŪēú Ūôėžěź žěźžč†žĚė Íįźž†ēžĚĄ žĚłžčĚŪēėÍ≥† ž°įž†ąŪēėŽäĒ Žä•Ž†•žĚĄ ÍłįŽ•īŽäĒ Í≤ɞ̥ Ž™©ŪĎúŽ°ú ŪēúŽč§[40]. žĚī žĻėŽ£ĆŽäĒ žĚľŽįėž†ĀžúľŽ°úŽäĒ 3ÍįúžõĒÍįĄ ŪöĆŽčĻ 90-120Ž∂Ą ž†ēŽŹĄžĚė žĄłžÖėžĚĄ 9-12Ž≤ą ž†ēŽŹĄ žßĄŪĖČŪēėŽäĒ Í≤ÉžĚī Í∂ĆÍ≥†ŽźúŽč§[41]. žė•žčúŪ܆žč† Žč§ŪöĆ Ūą¨žó¨žĚė Í≤Ĺžöį, ŽÖłž∂úžĻėŽ£ĆžôÄ Ž≥ĎŪĖČŪēėžó¨ ŽĻĄÍįēžúľŽ°ú žė•žčúŪ܆žč†žĚĄ ŪēėŽ£®žóź ŽĎź Ž≤ą ŪėĻžĚÄ žĚľž£ľžĚľ žóź Ūēú Ž≤ąžĒ© ž£ľÍłįž†ĀžúľŽ°ú Ūą¨žó¨ŪēėžėÄŽč§. žĚľŪöĆ Ūą¨žó¨žôÄ ŽŹôžĚľŪēú 40 IUžĚė žö©ŽüČžúľŽ°ú 7žĚľžóźžĄú 8žĚľÍįĄ 1žĚľ 2ŪöĆ(BID)Ž°ú Ūą¨žó¨Ūēú ŽÖľŽ¨łžĚī 2Ūéł[A18,A20], ŽŹôžĚľŪēú žö©ŽüČžúľŽ°ú žĚľž£ľžĚľžóź 1Ž≤ąžĒ© 8ž£ľ ŽėźŽäĒ 10ž£ľžóź ÍĪłž≥źžĄú Ūą¨žó¨Ūēú žóįÍĶ¨ÍįÄ 3Ūéł žěąžóąŽč§ [A21,A12,A22]. Ž™®Žď† ŽÖľŽ¨łžóźžĄú žė•žčúŪ܆žč†žĚÄ ŽĻĄÍįē žä§ŪĒĄŽ†ąžĚīŽ•ľ žā¨žö©Ūēėžó¨ Ūą¨žó¨ŽźėžóąŽč§. ŽĻĄÍįēžúľŽ°ú Ūą¨žó¨ŪēėŽäĒ žė•žčúŪ܆žč†žĚė ŽįėÍįźÍłįŽäĒ ŽĆÄŽěĶ 2-4žčúÍįĄ ž†ēŽŹĄžĚīŽ©į, Ūėąž§Ď žĶúÍ≥† ŽÜ掏ĄŽ•ľ Žč¨žĄĪŪēėŽäĒŽćį 30-45Ž∂Ą ž†ēŽŹĄ žÜĆžöĒŽźúŽč§[42]. ÍĶ≠žÜĆ ž£ľžā¨žóź ŽĻĄŪēī Ž∂ĄŪēīžÜ掏Ąžóź ŽĆÄŪēú ŪôēžāįžÜ掏ĄžĚė ŽĻĄÍįÄ žĽ§žĄú, ž§Ďž∂Ē žč†Í≤ĹÍ≥Ą Íłįž†Ąžóź ŽĻ†Ž•īÍ≥† ÍīĎŽ≤ĒžúĄŪēėÍ≤Ć žěĎžö©ŪēėÍłįžóź[43,44], Í≥†žįįŪēú Ž™®Žď† žóįÍĶ¨žóźžĄú ŽĻĄÍįēžĚĄ ŪÜĶŪēī Ūą¨žó¨Ūēú Í≤ÉžúľŽ°ú ŪĆźŽč®ŽźúŽč§. ŽėźŪēú, ŽĻĄÍįē ž†źŽßČžúľŽ°ú žė•žčúŪ܆žč†žĚĄ Ž∂Ąžā¨Ūēėžó¨ Ūą¨žó¨ŪēėŽäĒ Žį©Ž≤ēžĚÄ ŽĻĄžĻ®žäĶž†ĀžĚīŽĚľ, Ž∂ąŪéłÍįźžĚī ž†ĀÍ≥†, žā¨žö©žĚī ÍįĄŪéłŪēėžó¨, žĚľŽįėž†ĀžúľŽ°ú ŽÜížĚÄ žąúžĚĎŽŹĄŽ•ľ Ž≥īžĚłŽč§[42,45].
žė•žčúŪ܆žč† Žč§ŪöĆŪą¨žó¨Ūēú žóįÍĶ¨ 5Ūéł ž§Ď 3Ū鳞󟞥ú žā¨ŪöĆŪĖČŽŹô žł°ž†ē žßÄŪĎú(CAPS-5, PCL-5)ÍįÄ ÍįúžĄ†ŽźėžóąŽč§[A21,A12,A22]. ŽÖłž∂úžĻėŽ£ĆžôÄ žė•žčúŪ܆žč† žĻėŽ£ĆŽ•ľ 10ž£ľÍįĄ Ž≥ĎŪĖČŪēú žóįÍĶ¨[A21]žóźžĄú ŽĆÄž°įÍĶįžóź ŽĻĄŪēīžĄú CAPS-5 ž†źžąėŽäĒ 67% ÍįźžÜĆŪĖąžúľŽ©į, PCL-5 ž†źžąėŽäĒ 61% ÍįźžÜĆŪĖąŽč§. ŽÖłž∂úžĻėŽ£ĆžôÄ žė•žčúŪ܆žč† žĻėŽ£ĆŽ•ľ 10ž£ľÍįĄ Ž≥ĎŪĖČŪēú žóįÍĶ¨[A22]žóźžĄúŽŹĄ ŽĆÄž°įÍĶįÍ≥ľ žč§ŪóėÍĶį Ž™®ŽĎź ž¶ĚžÉĀžĚī ÍįźžÜĆŪēėžėÄžúľŽāė(CAPS-5,: žč§ŪóėÍĶį 47%, ŽĆÄž°įÍĶį 34% ÍįźžÜĆ, PCL-5: žč§ŪóėÍĶį 59%, ŽĆÄž°įÍĶį 42% ÍįźžÜĆ), žč§ŪóėÍĶįžóźžĄú ŽćĒ žú†žĚėŽĮłŪēú ÍįźžÜĆ Í≤įÍ≥ľŽ•ľ Ž≥īžėÄŽč§. ŽėźŪēú žĚī žóįÍĶ¨žóźžĄúŽäĒ, Ūėąž§Ď žė•žčúŪ܆žč† ŽÜ掏ĄŽ•ľ žł°ž†ēŪēėžėÄŽäĒŽćį, ŽĎź Í∑łŽ£Ļ Ž™®ŽĎźžóźžĄú Ūėąž§Ď žė•žčúŪ܆žč† ŽÜ掏ĄÍįÄ ÍįźžÜĆŪēėžėÄžßÄŽßĆ, ž¶ĚžÉĀ žč¨ÍįĀŽŹĄ ÍįźžÜĆžôÄŽäĒ ÍīÄŽ†®žĄĪžĚī žóÜžóąŽč§. ŽÖłž∂úžĻėŽ£ĆžôÄ žė•žčúŪ܆žč†žĚĄ Ž≥ĎŪĖČ Ūą¨žó¨Ūēú 2ŪéłžĚė žóįÍĶ¨žóźžĄú ž¶ĚžÉĀ ÍįúžĄ† Ūö®Í≥ľÍįÄ Ž≥īÍ≥†ŽźėžĖī, žč¨Ž¶¨žĻėŽ£Ćžóź ŽĆÄŪēú žė•žčúŪ܆žč†žĚė Ž≥īž°įžĻėŽ£Ćž†úŽ°úžĄúžĚė ÍįÄŽä•žĄĪžĚĄ ž≤ėžĚĆžúľŽ°ú ŪôēžĚłŪēėžėÄŽč§[A21,A22]. Í∑łŽü¨Žāė, Flanagan ŽďĪ[A12]žĚė žóįÍĶ¨žóźžĄúŽäĒ ŽÖłž∂ú žĻėŽ£ĆžôÄ Ž≥ĎŪĖČ Ūą¨žó¨Ūēú žė•žčúŪ܆žč†žĚė žčúŽĄąžßÄ Ūö®Í≥ľÍįÄ Ž≥īÍ≥†ŽźėžßÄ žēäžēĄ žēĄžßĀ Í≤įŽ°†žĚĄ ŽāīŽ¶¨ÍłįžóźŽäĒ Ž∂ąž∂©Ž∂ĄŪēėŽč§.
Žč§ŪöĆ Ūą¨žó¨ žóįÍĶ¨ 5Ū鳞󟞥ú Ūö®Í≥ľŪŹČÍįÄ žßÄŪĎúŽ°ú CAPS-5, PCL-5 ÍįôžĚÄ žā¨ŪöĆŪĖČŽŹôž†Ā žßÄŪĎúŽ•ľ žł°ž†ēŪēú žóįÍĶ¨ 4Ūéł, žč¨ŽįēŽ≥ÄžĚīŽŹĄ, ŪÉÄžē° žĹĒŽ•īŪčįžÜĒ, Ūėąž§Ď žė•žčúŪ܆žč† ŽďĪ žÉĚŽ¨ľŪĎúžßĞ쟎•ľ žł°ž†ēŪēú žóįÍĶ¨ÍįÄ 1Ūéł žěąžóąžúľŽāė, ŽáĆžėĀžÉĀžĚĄ žł°ž†ēŪēėžó¨ ŪŹČÍįÄŪēú žóįÍĶ¨ŽäĒ žóÜžóąŽč§. žĶúÍ∑ľ PTSD ŪôėžěźžóźžĄú ŽáĆžĚė ÍĶ¨ž°įž†Ā Ž≥ÄŪôĒŽŅźŽßĆ žēĄŽčąŽĚľ žēąž†ē žÉĀŪÉúžĚė ŽáĆ žóįÍ≤įŽßĚ ŽėźŽäĒ žąėŪĖČ Í≥ľž†ú žčú ŽāėŪÉÄŽāėŽäĒ ŽáĆ ŪôúžĄĪŪôĒ Ž∂ÄžúĄÍįÄ Žč§žĖĎŪēėÍ≤Ć Ž≥īÍ≥†ŽźėÍ≥† žěąžĖī, PTSD žĻėŽ£ĆžēĹŽ¨ľžĚė Ūö®Í≥ľ ŪŹČÍįÄŽ•ľ Ūē† ŽēĆ, ŽáĆžĚė ÍĶ¨ž°įž†Ā¬∑ÍłįŽä•ž†Ā Ž≥ÄŪôĒŽ•ľ ŪŹČÍįÄŪē† ŪēĄžöĒÍįÄ žěąŽč§[46]. Zuiden ŽďĪ[A18]žĚė žóįÍĶ¨žóźžĄúŽäĒ žė•žčúŪ܆žč† Ūą¨žó¨ ŪõĄ žč§ŪóėÍĶįÍ≥ľ ŽĆÄž°įÍĶį Ž™®ŽĎź CAPS ž†źžąėÍįÄ ŪēėŽĚĹŪĖąžßÄŽßĆ, Í∑łŽ£Ļ ÍįĄžĚė žú†žĚėŽĮłŪēú žį®žĚīÍįÄ ŽāėŪÉÄŽāėžßÄ žēäžēėŽč§. Í∑łŽü¨Žāė, CAPS ž†źžąė 45ž†źžĚĄ Íłįž§ÄžúľŽ°ú ž§Ďž¶Ě ŽėźŽäĒ Í≤Ĺž¶Ě ŪôėžěźÍĶįžúľŽ°ú Ž∂ĄŽ•ėŪēėžó¨ ÍīÄžįįŪēú Í≤įÍ≥ľ, ž§Ďž¶Ě ŪôėžěźÍĶįžóźžĄú Í≤Ĺž¶Ě Ūôėžěźžóź ŽĻĄŪēī žÉĀŽĆÄž†ĀžúľŽ°ú žú†žĚėŽĮłŪēú ž†źžąė ÍįźžÜĆÍįÄ ž∂Ēž†Ā ÍīÄžįįžĚė Í≤įÍ≥ľŽ°ú ŽāėŪÉÄŽāė, žė•žčúŪ܆žč†žĚė PTSD ž§Ďž¶Ě Ūôėžěźžóź ŽĆÄŪēīžĄú žě•ÍłįÍįĄ Ž≥īŪėł Ūö®Í≥ľ ÍįÄŽä•žĄĪžĚĄ žčúžā¨ŪēėžėÄŽč§. Engel ŽďĪ[A20]žĚė žóįÍĶ¨žóźžĄúŽäĒ Ž≥īž°įž†ĀžĚł Ž≥ÄžąėŽ°úžĄú PTSDžĚė ž¶ĚžÉĀžĚĄ ÍīÄžįįŪēėžėÄŽäĒŽćį, žė•žčúŪ܆žč†žĚĄ Ūą¨žó¨Ūē®žóź ŽĒįŽĚľžĄú CAPS ž†źžąėÍįÄ ÍįźžÜĆŪēėžėÄžĚƞ̥ Ž≥īžėÄŽč§.
žė•žčúŪ܆žč†žĚĄ žĻėŽ£Ćž†úŽ°úžĄú žā¨žö©ŪēėÍłį žúĄŪēīžĄú Í≥†Ž†§Ūēīžēľ Ūē† Ž™á ÍįÄžßÄ Ž≥ÄžąėÍįÄ ž°īžě¨ŪēúŽč§. žöįžĄ†, žė•žčúŪ܆žč†žĚÄ žĄĪŽ≥Ąžóź ŽĒįŽĚľ, žó¨žĄĪžĚīŽĚľŽŹĄ ÍįÄžěĄÍłį žó¨žĄĪÍ≥ľ ŪŹźÍ≤ĹÍłį žó¨žĄĪžóź ŽĒįŽĚľ žė•žčúŪ܆žč† Ūėąž§Ď ŽÜ掏Ą žį®žĚīÍįÄ ž°īžě¨ŪēúŽč§. Žā®ŽÖÄžĚė Ūėąž§Ď žė•žčúŪ܆žč† ŽÜ掏ĄŽäĒ 1-4 pmol/L (1.25-5 pg/mL)Ž°ú žēĆŽ†§ž†ł žěąÍ≥†, žó¨žĄĪžóźžĄúŽŹĄ ŽįįŽěÄÍłį žĶúŽĆÄžĻė(ovulatory peak) ŽÜ掏ĄŽäĒ 4-8 pmol/L (5-10 ng/mL) ž†ēŽŹĄŽ°ú žÉĀžäĻŪēėÍ≥†[47], ŪŹźÍ≤ĹÍłį žó¨žĄĪžĚī ÍįÄžěĄÍłį žó¨žĄĪŽ≥īŽč§ žė•žčúŪ܆žč†žĚė Ūėąž§Ď ŽÜ掏ĄÍįÄ ŽāģŽč§Í≥† Ž≥īÍ≥†ŽźėžóąŽč§[48]. ŽėźŪēú 90Ž™Ö(Žā®ŽÖÄ ŽĻĄžú® ŽŹôžĚľ, ŪŹČÍ∑† žóįŽ†Ļ 34.9¬Ī6.2žĄł)žĚĄ ŽĆÄžÉĀžúľŽ°ú žĄĪŽ≥Ąžóź ŽĒįŽ•ł žė•žčúŪ܆žč† žąėžĻėŽ•ľ ž°įžā¨Ūēú žóįÍĶ¨žóźžĄú žó¨žĄĪžĚī Žā®žĄĪŽ≥īŽč§ žė•žčúŪ܆žč†žĚė Ūėąž§Ď ŽÜ掏ĄÍįÄ žú†žĚėž†ĀžúľŽ°ú ŽÜížēėžĚƞ̥ ŪôēžĚłŪēėžėÄŽč§(4.53 pg/mL vs 1.53 pg/mL). žė•žčúŪ܆žč†žĚÄ Í∑ľžú°ž°įžßĀžĚė ž†Āž†ąŪēú žě¨žÉĚÍ≥ľ Ūē≠žÉĀžĄĪ žú†žßÄžóź ŪēĄžöĒŪēú ŪėłŽ•īŽ™¨žĚīŽĮÄŽ°ú, ŽāėžĚīÍįÄ Žď¶žóź ŽĒįŽĚľ Í≥®Í≤©Í∑ľžĚī ÍįźžÜĆŪēėŽ©ī Ūėąž§Ď žė•žčúŪ܆žč† ŽÜ掏ĄŽŹĄ žĚīžóź ŽĒįŽĚľ ÍįźžÜĆŪēėŽäĒ Í≤ÉžúľŽ°ú žēĆŽ†§ž†ł žěąŽč§[49]. Ūėąžē°Í≥ľ ŪÉÄžē°žóźžĄú žė•žčúŪ܆žč† ŽÜ掏ĄŽ•ľ žł°ž†ēŪēú Eidelman ŽďĪ[A2]žĚė žóįÍĶ¨žóźžĄúŽŹĄ Ž∂ĄžĄĚ ž†Ą ž∂Ēž∂ú Í≥ľž†ēžĚī Ž™ÖŪôēŪēėÍ≤Ć Íłįžą†ŽźėžßÄ žēäžĚÄ ž†úŪēúž†źžĚĄ Ž≥īžėÄŽč§. ŽĒįŽĚľžĄú žė•žčúŪ܆žč†žĚė PTSD žĻėŽ£Ć Ūö®Í≥ľŽ•ľ ŪŹČÍįÄŪē† ŽēĆŽäĒ žĄĪŽ≥Ą, ŽāėžĚī ŽďĪžĚĄ Í≥†Ž†§Ūēú žóįÍĶ¨žĄ§Í≥ĄžôÄ Ūē®ÍĽė Ž∂ĄžĄĚŽį©Ž≤ēžĚĄ Ž™ÖŪôēŪēėÍ≤Ć ž†úžčúŪē† ŪēĄžöĒÍįÄ žěąŽč§.
Ž≥ł žóįÍĶ¨Ž•ľ ŪÜĶŪēī, 13ŪéłžĚė žóįÍĶ¨žóźžĄú, ŽŹôžĚľŪēú ÍįĀ žč§Ūóė Žč®žúĄ(ŪĒľŪóėžěź)ÍįÄ Žč§Ž•ł ÍłįÍįĄ ŽŹôžēą Žč§Ž•ł žĻėŽ£ĆŽ•ľ ŽįõŽäĒ žóįÍĶ¨ ŽĒĒžěźžĚłžĚł ÍĶźžį®žčúŪóė ŽĒĒžěźžĚł(crossover design) ŪėĻžĚÄ ŪĒľŪóėžěź Žāī(within subject) žĄ§Í≥ĄŽ•ľ ŪÜĶŪēī ŪĒľŪóėžěź žā¨žĚīžóź ŽįúžÉĚŪē† žąė žěąŽäĒ žĄĪŽ≥Ą, žóįŽ†Ļ ŽďĪžĚė žį®žĚīŽ°ú žĚłŪēú Í∑łŽ£Ļ ÍįĄžĚė žį®žĚīŽ•ľ ž§ĄžĚīÍ≥†žěź Ūēú ŽÖłŽ†•žĚī ŪôēžĚłŽźėžóąŽč§. žĚīŽäĒ žčúŪóė ÍłįÍįĄ ŽŹôžēą ŪĒľŪóėžěźÍįÄ ŪēėŽāėžĚė žĻėŽ£Ć ŽėźŽäĒ ž§Ďžě¨Ž•ľ ŽįõŽäĒ ŪŹČŪĖČ ŽĒĒžěźžĚł(parallel design)žĚł ŪĒľŪóėžěź ÍįĄ žĄ§Í≥Ą(between-subject)Ž≥īŽč§ žĻėŽ£ĆŪö®Í≥ľŽ•ľ ŽćĒ Ūö®žú®ž†ĀžúľŽ°ú ŽĻĄÍĶźŪē† žąė žěąžúľŽ©į, ŽßĆžĄĪ žßąŽ≥ĎžĚīÍĪįŽāė žĻėŽ£ĆžēĹžĚī ž°īžě¨ŪēėžßÄ žēäŽäĒ žěĄžÉĀžčúŪóė žóįÍĶ¨žóź ž†ĀŪē©ŪēėŽč§Í≥† žēĆŽ†§ž†ł žěąŽč§[50].
ŽßąžßÄŽßČžúľŽ°ú, žė•žčúŪ܆žč†žĚė žě•Íłį Ūą¨žó¨žóź ŽĒįŽ•ł žēąž†ĄžĄĪžóź ŽĆÄŪēī Ž≥īÍ≥†ÍįÄ Ž∂Äž°ĪŪē®žĚĄ Ž≥ł žóįÍĶ¨Ž•ľ ŪÜĶŪēī ŪôēžĚłŪēėžėÄŽč§. Žč§ŪöĆ Ūą¨žó¨Ž•ľ žčúŪĖČŪēú ŽÖľŽ¨łžóźžĄú žĶúžÜĆ 8žĚľžóźžĄú žĶúŽĆÄ 10ž£ľÍĻĆžßÄžĚė Ūą¨žó¨ ÍłįÍįĄ ŽŹôžēą, ŪėĻžĚÄ žĚīŪõĄžĚė 6ÍįúžõĒ ž†ēŽŹĄ ž∂Ēž†ĀÍīÄžįįÍĻĆžßÄ, ÍĶ¨ž≤īž†ĀžĚł Ž∂ÄžěĎžö© žł°ž†ēžóź ŽĆÄŪēú Ž≥īÍ≥†žóÜžĚī Ž∂ÄžěĎžö©žĚī žóÜžóąŽč§ŽäĒ žĖłÍłČŽßĆ ŪēėžėÄŽč§. ŽĒįŽĚľžĄú ŪĖ•ŪõĄ žßĄŪĖČŽź† žė•žčúŪ܆žč†žĚė žĻėŽ£Ćž†Ā Ūö®Í≥ľžóź ŽĆÄŪēú ŽĆÄÍ∑úŽ™® žěĄžÉĀžčúŪóėžóźžĄúŽäĒ žĄĪŽ≥ĄÍ≥ľ ÍįÄžěĄÍłį žó¨Ž∂Ä, ŽāėžĚī, žēąž†ĄžĄĪ ŽďĪžĚė Ž≥ÄžąėŽ•ľ Í≥†Ž†§Ūē† ŪēĄžöĒÍįÄ žěąŽč§. Žėź, ŪéłŪĖ•žĚė ÍįÄŽä•žĄĪžĚī žĽ§žßÄŽäĒ Í≤Ĺžöį RCT Í≤įÍ≥ľžóź ŽĆÄŪēú Í≥ľžě•Žźú ŪēīžĄĚžĚė žó¨žßÄŽ•ľ ž§Ą žąė žěąÍłįžóź[51], ŪéłŪĖ•žĚė žúĄŪóė(Risk of bias)žĚī ŽāģŽŹĄŽ°Ě žóįÍĶ¨Ž•ľ žĄ§Í≥ĄŪē† ŪēĄžöĒÍįÄ žěąŽč§. ŪäĻŪěą, ž†Ąžāį Žāúžąė žÉĚžĄĪÍłį, ŽāúžąėŪĎúŽāė ŽŹôž†Ą ŽćėžßÄÍłį ŽďĪžĚė Žį©Ž≤ēžĚĄ ŪŹ¨Ūē®Ūēėžó¨ ŽāúžąėžóīžĚĄ žÉĚžĄĪŪēėÍ≥†, ž§Ďžč¨ Ūē†ŽčĻ(Central allocation), žĚľŽ†® Ž≤ąŪėłÍįÄ Žß§Í≤®žßĄ ŽīȞ̳ ŽīČŪą¨(Sequential numbered sealed envelope, SNOSE) ŽďĪžĚĄ žā¨žö©Ūēėžó¨ Žįįž†ēžĚÄŽčȞ̥ ž≤†ž†ÄŪēėÍ≤Ć ŪēėÍ≥† žĚīŽ•ľ Ūą¨Ž™ÖŪēėÍ≤Ć ŽÖľŽ¨łžóź Ž≥īÍ≥†Ūēīžēľ ŪēúŽč§. ŽėźŪēú Í≥ĄžłĶŪôĒÍįÄ ŪēĄžöĒŪēú žóįÍĶ¨žóźžĄúŽäĒ ŽłĒŽ°Ě ŽěúŽć§ ŽĒĒžěźžĚłžĚĄ Í≥†Ž†§Ūē† žąė žěąžĚĄ Í≤ÉžĚīŽč§.
Í≤į Ž°†
ž≤īÍ≥Ąž†ĀžĚł Ž¨łŪóĆÍ≥†žįįžĚĄ ŪÜĶŪēī žė•žčúŪ܆žč†žĚė Ūą¨žó¨ž°įÍĪīÍ≥ľ Ūö®Í≥ľ ŪŹČÍįÄžßÄŪĎúŽ•ľ Ž∂ĄžĄĚŪē®žúľŽ°úžć® PTSD žĻėŽ£Ćž†úŽ°úžĄúžĚė žė•žčúŪ܆žč†žĚė ÍįÄŽä•žĄĪžĚĄ ŪôēžĚłŪēėÍ≥†žěź žąėŪĖČŪēú Í≤įÍ≥ľ, ŽÖłž∂úžĻėŽ£ĆžôÄ žė•žčúŪ܆žč†žĚĄ Ž≥ĎŪĖČ Ūą¨žó¨Ūēú 2ŪéłžĚė žóįÍĶ¨žóźžĄú ž¶ĚžÉĀÍįúžĄ† Ūö®Í≥ľÍįÄ Ž≥īÍ≥†Žź®žĚĄ ŪôēžĚłŪēėžó¨ PTSD žč¨Ž¶¨žĻėŽ£Ćžóź ŽĆÄŪēú žė•žčúŪ܆žč†žĚė Ž≥īž°įžĻėŽ£Ćž†úŽ°úžĄúžĚė ÍįÄŽä•žĄĪžĚĄ ž≤ėžĚĆžúľŽ°ú ŪôēžĚłŪēėžėÄŽč§. Í∑łŽü¨Žāė, žė•žčúŪ܆žč†žĚĄ Žč§ŪöĆ Ūą¨žó¨Ūēú ŽÖľŽ¨łžĚė žąėÍįÄ 5ŪéłžúľŽ°ú ž†ĀÍ≥†, Í∑ł Ūö®Í≥ľŽ•ľ žě•Íłįž†ĀžúľŽ°ú ž∂Ēž†ĀŪēú žóįÍĶ¨ÍįÄ Ž∂Äž°ĪŪēėžó¨ ŪõĄžÜć žóįÍĶ¨ÍįÄ ŪēĄžöĒŪē®žĚĄ ŪôēžĚłŪēėžėÄŽč§. PTSDžóź ŽĆÄŪēú žė•žčúŪ܆žč†žĚė Ūö®Í≥ľŽ•ľ ŪŹČÍįÄŪēėÍłį žúĄŪēīžĄúŽäĒ žĄĪŽ≥Ą, žóįŽ†Ļ ŽďĪžĚė Ž≥ÄžąėŽ•ľ Í≥†Ž†§Ūēīžēľ ŪēúŽč§. ŪēėžßÄŽßĆ Ž≥ł ž≤īÍ≥Ąž†Ā Í≥†žįį žóįÍĶ¨žóźžĄúŽäĒ žĚīŽü¨Ūēú Ž≥ÄžąėŽď§žĚė žėĀŪĖ•Ž†•žóź ŽĆÄŪēīžĄúŽäĒ ŪÜĶž†úŪēėžßÄ Ž™ĽŪēėžėÄŽč§. ŽĒįŽĚľžĄú Ūö®Í≥ľžĄĪžóź žėĀŪĖ•žĚĄ ž£ľŽäĒ Ž≥ÄžąėŽď§žóź ŽćĒŪēī žā¨ŪöĆŪĖČŽŹôŪēôž†ĀžĚł ŪŹČÍįÄŽŅźŽßĆ žēĄŽčąŽĚľ žÉĚŽ¨ľŪēôž†ĀžßÄŪĎúžôÄ žč†Í≤ĹžėĀžÉĀŪēôž†ĀžßÄŪĎúŽ•ľ ž≤īÍ≥Ąž†ĀžúľŽ°ú Í≥†Ž†§Ūēú ŽĆÄÍ∑úŽ™® žěĄžÉĀžčúŪóė žóįÍĶ¨ÍįÄ ŪēĄžöĒŪēėŽč§Í≥† žā¨Ž£ĆŽźúŽč§. ŽėźŪēú Ž≥ł ŽÖľŽ¨łžóźžĄúŽäĒ PTSD ŪôėžěźŽď§žóź ŽĆÄŪēú žė•žčúŪ܆žč†žĚė Žč§ŪöĆ ŽĻĄÍįē Ūą¨žó¨ÍįÄ žč¨Ž¶¨žĻėŽ£ĆžôÄ Ž≥ĎŪĖČŽźėžóąžĚĄ ŽēĆ žěĄžÉĀž†Ā Ūö®Í≥ľŽ•ľ ŽįúŪúėŪē† žąė žěąžĚĄ Í≤ÉžĚīŽĚľÍ≥† ŪĆĆžēÖŪēėžėÄŽč§. PTSDžóź ŽĆÄŪēú ŪôėžěźŽď§žĚė žĻėŽ£Ć žĚīŪĖČŽ•†žĚī ŽāģžĚƞ̥ Í≥†Ž†§ŪēėžėĞ̥ ŽēĆ, žěźÍįÄŪą¨žó¨ŽĚľŽäĒ žĻėŽ£ĆžĚė žö©žĚīžĄĪžĚī žĚī Ž¨łž†úŽ•ľ ÍįúžĄ†Ūēī ž§Ą žąė žěąžĚĄ Í≤ÉžĚīŽĚľÍ≥† žā¨Ž£ĆŽźúŽč§. žĚīŽäĒ PTSD ŪôėžěźŽď§žóź ŽĆÄŪēú ÍįĄŪėł žąėŪĖČ žĄĪÍ≥ľžĚė ŪĖ•žÉĀžĚīŽĚľŽäĒ žł°Ž©īžóźžĄú žĚėžĚėŽ•ľ ÍįĖŽäĒŽč§.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



